Two-dose coronavirus vaccine regimens will make it harder to inoculate America
Health & BeautyNov 28. 2020On the road outside rural Wessington Springs, S.D., where 1 in 37 people had the virus this month. MUST CREDIT: Photo for The Washington Post by Jenn Ackerman
By The Washington Post · Frances Stead Sellers · NATIONAL, HEALTH, SCIENCE-ENVIRONMENT, HEALTH-NEWS, HEALTH-FEATURES
When Molly Howell talks about the two-shot regimen needed to vaccinate residents of North Dakota’s 210 long-term-care facilities against the coronavirus, she sounds like a general mobilizing a massive air lift without knowing how many planes she will have.
As the state’s immunization program manager, Howell is on top of mass vaccinations for seasonal flu, essentially a one-stop shot. And she is well versed in serial immunizations, like the two-step shingles shots. But for the current coronavirus vaccines, which require two injections spaced either three or four weeks apart, she anticipates clinicians having to make many more than two visits to facilities. Will health-care workers be considered a high-priority group and thus scheduled for vaccination sooner than at-risk residents? How should shift workers be accommodated? And what about the many people who move in or out of facilities in the window between shots?
“It definitely will be an iterative process,” Howell said, as she multiplied those problems through jails, group homes and homeless shelters, wondering how not to waste precious doses if somebody doesn’t show up as expected for their second shot, leaving a precious vial in the refrigerator.
“Do you use second doses for first doses?” Howell speculated.
As the nation gears up to vaccinate tens of millions of Americans against the novel coronavirus, public health officials like her are facing novel dilemmas, driven by the urgency of the pandemic, the fact that only a small minority may have immunity from prior exposure and by the vaccine available at each site, with the differing intervals between shots depending on the manufacturer.
They will need to keep track of people who have received one dose in order to send a reminder about the need to return a few weeks later. They worry that the first vaccine may make people feel just sick enough that they won’t want to go through the ordeal again. And they foresee hitches if people get their first dose at, say, Walgreens and go to CVS for their second, or, worse still, if they cross state borders, moving from one health department’s registration system to another.
“Two doses more than doubles the logistical challenges of administering the vaccines,” said Jeffrey Duchin, health officer for public health in Seattle and King County, Wash. “The moving parts have to align.”
A two- or three-dose dose regimen is routine for building immunity against many illnesses, but it is unprecedented in a pandemic when the public health goal is to vaccinate 60 to 70% of the population within months to reach herd immunity and stop the virus’s spread.
“This is the only time we’ve faced a serious, immediate threat to the entire population that requires a two-dose vaccine,” said Kelly Moore of the Immunization Action Coalition, who was director of Tennessee’s program in 2009 during the H1N1 pandemic and recalls her relief when she learned everyone but young children would need only one shot.
That was possible because unlike covid-19, which is caused by a novel virus, an influenza similar to H1N1 had previously circulated in humans giving many people partial immunity. Clinical trials showed that protection was afforded with only one injection.
With Ebola, Moore said, both single- and two-dose vaccines exist and experts have been figuring out how best to deploy them both in and around outbreaks, depending on the availability of supplies.
It’s not unusual for a vaccine to require re-upping in order to provoke the immune system to respond more effectively. The classic schedule for vaccines that target proteins like the spike protein on the surface of this coronavirus, Moore said, is three shots – “prime, prime, boost” – with the second and third shots coming one and six months after the first injection. Each of the first two shots primes the immune system and is typically followed by a modest drop-off in antibodies. The third shot, usually at least six months after the first one, can give long-term protection by boosting the immune system’s memory cells, which by that point have matured and are ready to respond.
It’s not yet clear whether any of the new coronavirus vaccines in the pipeline will ultimately work best with a third shot capable of boosting long-term protection.
“Memory cells increase stepwise during at least six months,” said Claire-Anne Siegrist, a professor of vaccinology at the University of Geneva and head of the World Health Organization’s Collaborating Center for Vaccine Immunology. The urgency of the increasing infection rates and death tolls has led to the promotion of an immediate two-shot solution.
“In a ramping pandemic, where efficacy should be elicited as rapidly as possible, giving two primary vaccine doses and following to see whether and when a booster might be needed is a most reasonable choice,” she said.
It’s also possible that fewer doses may prove sufficient.
“For all we know, all these two-dose vaccines may work in one dose,” Duchin said.
Data will be gathered as populations are immunized, providing further information about how best to vanquish this particular disease.
“I think we have to learn what is needed to keep immunity,” said Bruce Gellin, president of global immunization at the Sabin Vaccine Institute, fine-tuning strategies and policies based on the evolving science, with the potential for revaccination in the future, as with the annual flu vaccine.
“There are a lot of missing data points,” said John Brownstein, chief innovation officer at Boston Children’s Hospital, who runs Vaccine Finder, a system developed by Google a decade ago to help deploy the H1N1 vaccine.
The Vaccine Finder is designed to help people find providers of vaccines, from flu to shingles, close to where they live. The system doesn’t collect personal data, however, which would be necessary to send out reminders to individuals about a second coronavirus shot, for example.
“Right now, it’s a one-way push,” said Brownstein, who described his ambitions to rebuild the infrastructure so people could receive updates and information about scheduled vaccines.
The challenges of registering individuals and reminding them electronically about their second shots are daunting, said Sacramento County Health Director Peter Beilenson, who like Howell is concerned about the potential inefficiency of staggered staff and residents’ immunizations in long-term-care and other residential facilities.
The two-shot emergency schedule will upend the way many health departments have organized mass vaccination programs in recent years. For a decade, the Vanderbilt University School of Medicine has developed a program to immunize students, faculty, staff and volunteers against the flu – a one-shot-and-you’re-done deal that has succeeded in immunizing as many as 15,000 people in a single day.
Many of those efficiencies won’t be possible with the two-shot regime.
“It does impact staffing resources” at a time when health-care workers are already stretched thin, said Vanderbilt infectious-disease chief Thomas Talbot.
The coronavirus vaccines may give headaches, fevers and other unpleasant symptoms – all good signs of the body’s immune system getting to work – but Talbot is concerned they may prevent people from returning for their second dose.
Moore, who has studied another painful vaccine – two-dose shingles shots – says she is heartened by the way a vast majority of people who are educated about what to expect come back for their second doses despite the discomfort.
“I am very encouraged that our experience with Shingrix is that motivated people will come back as long as they are properly prepared to do so,” Moore said.
And while the challenges ahead are daunting, Howell said she is glad to be able to think them through with other experts.
“It’s comforting that we are all in same position,” she said. “All of us are going to figure this out.”
By Syndication Washington Post, Bloomberg · Angelica LaVito · NATIONAL, HEALTH, HEALTH-NEWS
Large hospital systems are grappling with how best to decide which health-care workers will be vaccinated first for covid-19, a daunting task when it’s unclear which shots they’ll get, how many and when they’ll arrive.
The first covid-19 vaccine could be cleared for U.S. use as soon as next month, with Pfizer Inc. and BioNTech SE’s candidate already under review and Moderna Inc.’s shot not far behind. Federal officials, meanwhile, have signaled that health-care workers and older Americans at high risk should be vaccinated as step one in what could set off months of fraught decisions involving other key priority groups.
But following those initial guidelines could prove difficult. With 21 million health-care workers in the U.S., there almost certainly won’t be enough doses to reach them all at once. That’s forcing hospitals to categorize their workers based on best-guess distribution estimates, a task made even more complex for some systems by a patchwork state-by-state approach.
Minnesota’s Allina Health system, which employs 15,600 workers who have direct contact with patients in Minnesota and Wisconsin, is estimating it could get 3,000 to 4,000 doses initially. The plan: Prioritize those that interact directly with coronavirus patients by listing each worker by their job type and the units they work in.
“We’re looking at all employees, where they work, what their roles are and what their exposure risk is,” said Ryan Else, a doctor who is overseeing the coronavirus response in Allina Health’s hospitals.
Health systems that operate across state lines face an even bigger challenge. While states are taking cues from federal guidelines, they are developing their own priority lists, creating a situation where some employees in one state might get vaccinated before their peers in another.
“How fair does that feel to people in the same system?” said Amy Compton-Phillips, a doctor and chief clinical officer at Providence, which operates 51 hospitals, as well clinics and medical offices across seven states.
Like Allina, Providence also plans to vaccinate workers based on their roles in an attempt at fairness. The health system will notify workers when it’s their turn to get vaccinated. It is also creating an appeal process if people think groups were misclassified. “When things are in short supply, you make really hard decisions. They don’t feel good,” Compton-Phillips said.
Federal officials plan to initially send 6.4 million doses across the country, according to Gus Perna, Operation Warp Speed’s chief operating officer. More doses will then be sent out on a weekly basis with the goal of distributing 40 million doses by the end of the year, Perna said on a call with reporters Tuesday.
Shipments will be divvied up across states based on the size of their adult populations, and not in response to any virus surges, U.S. Department of Health and Human Services Secretary Alex Azar said on the call.
“We wanted to keep this simple, first because we’re seeing nationwide spread and susceptibility to the disease,” Azar said. “But also, once we pass through these initial tranches where we’re in much more of a scarcity situation, we’re eventually going to get to the point where it would need to be per capita. So instead of having multiple methodologies, we thought it best to keep it simple.”
Some health systems are taking a more granular approach in preparing for use of the shots.
Advocate Aurora Health Inc., with 26 hospitals and even more clinics and doctors across Illinois and Wisconsin, is identifying workers at greatest risk of severe illness, anticipating it will not receive enough doses to cover employees evenly. That means factoring in details like how prevalent the coronavirus is in a particular community, as well as employees’ risk factors, said Robert Citronberg, a doctor and executive medical director of infectious disease and prevention.
“We want to target as best as possible the people who are most likely to get severely ill from covid, and we know those are older people, people with underlying medical conditions,” Citronberg said.
New York’s Northwell Health, with 23 hospitals, has already compiled a spreadsheet of its 74,000 workers that categorizes them by their risk of catching the novel coronavirus on the job, according to Mark Jarrett, who is a doctor and the system’s chief quality officer.
Northwell’s calculation weighs how much employees interact with infected patients and, like Advocate Aurora, how prevalent the virus is in the community. That second data point could change at times, resulting in people working in areas with more spread being vaccinated first.
And Jarrett brings another issue to the table. He’s worried less about people clamoring for a vaccine and more about workers not wanting one, a fear other hospital executives across the country echoed.
Health systems already had to contend with anti-vaccination movements when concerns about the quick speed of covid-19 vaccine development further spooked workers, Providence’s Compton-Phillips said.
Allison Suttle, a doctor and chief medical officer of Sioux Falls, South Dakota-based Sanford Health, hopes clinical trial data will reassure the system’s workers. Internal surveys found more people said they would take a covid-19 vaccine after Pfizer and Moderna released early results showing their candidates were each around 95% effective.
“I’m optimistic, cautiously optimistic, and proud of our health-care workers that they’re willing to jump up, stick out their shoulder and get the vaccine,” Suttle said.
If and when the Food and Drug Administration authorizes vaccine candidates, the Centers for Disease Control and Prevention will make its final recommendations for whom to vaccinate. Members of the CDC’s immunization committee will review the data for clues on whether the formulas work better in some groups than others.
In the meantime, health systems will continue preparing as best they can. When asked whether Northwell knows how many doses it will receive, Jarrett laughed.
“Nope,” he answered. Any estimates are likely to change, Jarrett said, and even the smallest of fluctuations could make a big difference.
By Syndication Washington Post, Bloomberg · Suzi Ring, James Paton · NATIONAL, BUSINESS, HEALTH, HEALTH-NEWS
AstraZeneca’s covid-19 vaccine looks as if it’s headed for an additional global trial as the drugmaker tries to clear up uncertainty and confusion surrounding favorable results in its current study.
The company wants the new test to confirm the 90% efficacy rate that the shot showed in a portion of an existing trial, Chief Executive Officer Pascal Soriot said. It’s favoring that option rather than adding an arm to a separate study that’s already underway in the U.S.
Questions are mounting over one of the fastest-moving shots after the company acknowledged that a lower dosage level that appeared more effective resulted from a manufacturing discrepancy. The company and its partner, the University of Oxford, didn’t initially disclose the error and other key details, leading to concern over their transparency.
“Now that we’ve found what looks like a better efficacy we have to validate this, so we need to do an additional study,” Soriot said in his first interview since the data were released. It will probably be another “international study, but this one could be faster because we know the efficacy is high so we need a smaller number of patients.”
Soriot said he didn’t expect the additional trial to hold up regulatory approvals in the U.K. and European Union.
U.K. Health Secretary Matt Hancock asked the nation’s medical regulator to potentially bypass its E.U. counterpart and approve the supply of AstraZeneca’s vaccine to speed its deployment. Until the end of the year, when the U.K. exits a post-Brexit transition period, vaccines must be authorized by the European Medicines Agency. But on Friday, Hancock said he invoked a special rule allowing Britain’s regulator to authorize a temporary supply of the vaccine if the data is robust enough.
Clearance from the U.S. Food and Drug Administration may take longer because the regulator is unlikely to approve the vaccine on the basis of studies conducted elsewhere, especially given the questions over the results, Soriot said. Authorization in some countries is still expected before the end of the year, he said.
“The question for us was, will we need the U.S. data to get approval in the U.S. or can we get approval in the U.S. with international data, and it was never clear,” said Soriot, who is in quarantine after arriving in Australia. “Now with those results it’s more likely that we will need the U.S. data.”
Astra and its CEO are facing scrutiny as the drugmaker responds to growing confusion over the vaccine. The company’s late-stage data initially increased confidence that the world would soon have multiple shots to combat the pathogen, following positive reports from front-runners Pfizer Inc. and Moderna Inc. But scant disclosures and the manufacturing discrepancy have sparked doubts among scientists and investors.
Astra shares fell 0.8% by 8:57 a.m. in London trading Friday, bringing the decline this week to about 8% amid questions about the trial results.
Astra and Oxford reported Monday that a lower initial dose of the vaccine, followed by a full dose, produced a 90% efficacy rate in a smaller set of participants, compared with 62% for two full doses.
A day after the data were unveiled the head of Operation Warp Speed, the U.S. vaccine program, said that the regimen showing the higher level of effectiveness was tested in a younger population. He also said the half-dose was given to some people because of an error in the quantity of vaccine put into some vials. None of those details were disclosed in Astra or Oxford’s original statements.
Soriot disputed the idea that the half-dose regimen was an error, saying that after researchers realized the dosing discrepancy they formally changed the trial protocol with the blessing of regulators.
“I won’t tell you we expected the efficacy to be higher,” said Soriot. But “people call it a mistake — it’s not a mistake.”
The company has previously said it might add a new arm to its U.S. trial to test the lower dosage.
Astra and researchers have declined to provide more data ahead of a peer-reviewed analysis that is expected to be published in the coming weeks. Results have been submitted to an undisclosed journal, Astra said in a statement.
Astra’s is one of three vaccines that could be approved before the end of the year. Pfizer and Moderna, which have both created shots using messenger RNA, published data earlier this month that showed their vaccines were about 95% effective, and Pfizer has applied to U.S. regulators for emergency approval.
There’s added pressure on the Astra shot to succeed because it’s easier to store and the company is selling it at cost during the pandemic, which means many low- and middle-income countries are relying on it.
By The Washington Post · Tim Elfrink · NATIONAL, HEALTH, HEALTH-NEWS
Earlier this month, with coronavirus cases rising dramatically across Wyoming, a coalition of medical experts and nearly every county health officer in the state wrote to Republican Gov. Mark Gordon with an urgent demand: to issue a statewide mask mandate.
Gordon declined. While he has stressed the importance of wearing masks, he has also argued that it’s an individual choice to do so.
“It is incredibly important that we take personal responsibility for our actions and understand how those actions can implicate others,” Gordon said last month.
Now Gordon, 63, has tested positive for the virus, his office announced Wednesday. “He only has minor symptoms at this time and plans to continue working on behalf of Wyoming remotely,” Gordon’s office said in a news release.
Throughout the pandemic, a number of Republican governors have resisted mandating face coverings, with some questioning their effect – an echo of President Donald Trump’s dismissive attitude toward masks – and others, like Gordon, calling for personal responsibility. But in recent weeks, with the pandemic dramatically worsening and evidence mounting that mask mandates can reduce transmission, several have reversed course.
GOP-led states including Utah, West Virginia and North Dakota all recently tightened mask rules, and Iowa Gov. Kim Reynolds, a Republican who had previously called such rules “feel-good” measures, put a limited mandate into effect earlier this month.
Gordon, though, has held firm against any statewide mask rules even as Wyoming, like other states in the West and Midwest, has seen coronavirus cases increase significantly this fall. The state has now topped 30,000 cases and recorded at least 215 deaths, according to The Washington Post’s coronavirus tracker.
While some counties in Wyoming have issued local mask requirements, health experts say they’re often ignored – and enacting new rules on the county level hasn’t been easy.
When commissioners in Natrona County, which includes Casper, the state’s second-largest city, invited health officials to discuss a possible mask mandate this month, the meeting had to be adjourned early because of incessant heckling. Anti-mask protesters have repeatedly gathered at the state Capitol in Cheyenne as well.
On Nov. 12, Wyoming public health experts urged Gordon to reconsider a statewide mask rule. A letter signed by 21 county health officers and the heads of the state’s medical society and hospital association noted that recommendations alone weren’t driving enough people to mask up.
“Education and encouragement alone have not achieved desired outcomes. Our health care resources are becoming critically strained with hospitalizations and deaths increasing,” the letter said.
Last week, Gordon responded to the record case numbers by issuing new restrictions, including reducing the size of indoor and outdoor gatherings. And he urged residents to wear masks.
“The Governor reminded residents to practice the three Ws – wash your hands, watch your distance and wear a face covering,” his office said Nov. 19.
But Gordon again stopped short of issuing a mask mandate.
By The Washington Post · Brittany Shammas, Mark Guarino, Jacqueline Dupree · NATIONAL, HEALTH, HEALTH-NEWS For a few months, coronavirus-weary Chicago residents got a reprieve from the strict regulations that shuttered the nation’s third-largest city during the spring.
After infections plummeted in early June, restaurants welcomed diners back inside. Movie theaters, fitness centers and bowling alleys reopened their doors. And the barriers came down on the bike pathway along the city’s cherished lakefront.
But with new coronavirus cases surging beyond the springtime peak, Chicago is now hunkering down. Statewide measures have closed some businesses and limited the capacity at others, while officials are urging residents to stay home. Again.
“We’ve been through a heck of a lot this year,” Lori Lightfoot, the city’s Democratic mayor, said during a recent news conference. “And it’s not over.”
Across much of America, the picture is similar. Major metropolitan areas were the face of the pandemic before being overtaken by spikes in less populated parts of the country in September. Since then, the nation’s worst outbreaks have been concentrated in rural parts of the Upper Midwest.
Yet dramatic increases have been reported in many major American cities in recent weeks, with some being hit harder than they were during their previous peaks. Testing has greatly ramped up since the start of the pandemic, but that alone does not explain the growing caseloads.
“The dreaded fall wave, in many places, is upon us,” said Josh Michaud, an epidemiologist and associate director for global health policy at the nonprofit Kaiser Family Foundation. “And that includes in metropolitan areas.”
In Cook County, where Chicago is located, the seven-day average of new cases hit a record high of 4,654 on Nov. 17 – far outpacing the peak of 1,690 during the spring surge. Deaths are lower than the numbers seen in the spring but have climbed in recent weeks.
With winter approaching, business owners who stayed afloat by turning to outdoor service have been investing in heating lamps, hoping to keep customers coming even in temperatures that can drop below freezing.
Michelle Foik, co-owner of Eris Brewery & Cider House, said she saw the shutdown of indoor dining as inevitable. The facility’s patio has been “our saving grace,” she said, but she worries about what will happen this winter. She’s torn between relief that the rise in cases was met with more restrictions and concerned over the impact on her business.
“Believe me, we need the money,” Foik said. “We’re a start-up. We are investing in our future, but if this become a longtime shutdown, it just hurts everything.”
At NorthShore University HealthSystem, infectious-disease specialist Kamaljit Sandhu Singh said he and other health-care workers were “exhausted physically and mentally” as hospitalizations and intensive care unit admissions increased.
He said the pandemic reminded him of growing up during the Vietnam War: “I could never wrap my name around the number of soldiers’ lives lost, but the pictures were compelling.”
Cases are surging on Chicago’s West and Southwest sides, where the virus spread at a disproportionate rate in the spring and the majority of residents are Black or Latino. Kiran Joshi, senior medical officer at the Cook County Department of Public Health, said “a myriad of factors” play into why those areas are surging highest, but that a common attribute is that people there “experienced structural racism over decades.”
The second peak in Chicago mirrors those in metropolitan areas across the country. In recent weeks, counties home to cities including Philadelphia, Los Angeles, Detroit, Las Vegas and Minneapolis have seen new cases surpass their past highs. Miami-Dade County has been trending up again, while Salt Lake County is experiencing its first major peak of the pandemic, with cases and hospitalizations rising since early October.
In Maricopa County, which includes Phoenix, Valleywise Health “had a little breather” after the summer’s surge in Sun Belt states, said Michael White, the health system’s chief clinical officer. But the seven-day average of new cases, which hovered around 500 a day in late October, exceeded 2,000 on Monday.
“We’re hanging in there is how I would describe it,” White said. “Our biggest concern always is, as we continue to see this case count rise, that that certainly can lead to more folks needing hospitalization down the road, on top of a time where we usually see a higher rate of hospitalizations for non-covid-related illnesses.”
Phoenix-based Banner Health is projecting that 125 percent of the system’s licensed hospital beds will be full by the first week of December. Hospital administrators believe they have stocked up on enough personal protective equipment, ventilators and beds to weather the surge, Chief Clinical Officer Marjorie Bessel said during a news conference Tuesday. They worry most about staffing – they’ve hired nearly 1,000 health-care workers from out of state and are recruiting 900 more.
The health system always beefs up its staff for the winter months, Bessel said, but the coming weeks are expected to be markedly different from previous years and even the Sun Belt’s summer surge.
“The entire country is surging at the same time,” she said.
Health officials attribute the virus’s resurgence in cities to several factors, including eased restrictions, increased gatherings and what’s being called “covid fatigue.” Eight months into the pandemic, “there is no longer that sense of urgency,” said Mouhanad Hammami, chief health strategist in Wayne County, home to Detroit. “When you live with something, it is no longer urgent, and you tend to get desensitized to it.”
Some authorities in Chicago blamed rock-bottom hotel prices and the state-imposed indoor dining ban, suggesting it may have caused parties to relocate to hotel rooms or other spaces, such as Airbnb rentals. On Nov. 12, Lightfoot told reporters that current restrictions apply to both.
“I know the hotel industry was hit hard and is in many instances is on life support, but that cannot include parties,” she said. “I urge the hotel industry to be much more diligent about who is coming in. … People think it’s party time. It’s not.”
Officials in many hard-hit cities also point to increasingly widespread transmission across the United States, which has been reporting record-setting numbers of infections. Over the past week, the country had well over 150,000 new cases each day. Ahead of Thanksgiving, traditionally a time of significant travel and extended family get-togethers, health experts feared the number would only continue to climb.
“We would love to be that shining city on the hill where we’re avoiding all this,” said Philadelphia Department of Public Health spokesman James Garrow. “But I don’t know that anybody’s going to be able to avoid this.”
Mortality rates have improved from earlier in the pandemic – a change attributed to improved therapeutics and knowledge of how to handle covid-19, the disease caused by the virus. Still, authorities in areas that are seeing spiking infections have reacted with alarm, noting that the explosion in cases will inevitably drive up the death toll.
In Los Angeles County, where hospitalizations are up and deaths increased slightly last week, Public Health Director Barbara Ferrer on Friday described the data as looking “really bad right now” and added that the county had experienced “three terrible days in terms of case rates and increases in hospitalizations.” She said health officials were hoping deaths “don’t go up … as much as earlier in the pandemic.”
With rapidly rising case numbers has come a return to some of the restrictions of the spring. In Los Angeles, health officials suspended outdoor dining for the first time since May. They warned that a stay-at-home order could follow if the situation worsens.
Wayne County’s health department on Friday strongly recommended that schools shift to virtual instruction through mid-January, noting that the current wave “is at a level higher than the first peak in April 2020.”
Philadelphia on Nov. 20 imposed new “Safer at Home” restrictions, which required schools to shift to online learning, restaurants to suspend indoor dining, and gyms and indoor fitness classes to close. Movie theaters, casinos and bowling alleys were also shuttered and indoor gatherings of more than one household prohibited.
“The hope is that by implementing these restrictions as soon as we could – and we’re doing it ahead of at least a lot of surrounding counties and states – that we’ll be able to head off getting to a point where we outstrip our capacity and get to a point worse than we were in April,” Garrow said.
Months after the first shutdowns in the United States, a better understanding of how the coronavirus spreads means that this latest wave of restrictions can be more targeted, Michaud said. Authorities can focus on what is believed to carry the greatest risk of transmission: venues where people are crowded together indoors for extended periods of time.
“In the spring, we didn’t know a whole lot about the virus and exactly what were the activities that were the riskiest,” he said. “We know a whole lot more now. And that means that we don’t have to put in a Chinese-style lockdown to have an effect on transmission. You can be much more surgical in your approach.”
But among some already battered by earlier shutdowns, the new restrictions drew frustration.
The Illinois Restaurant Association released a statement objecting to the state’s ban on indoor dining, arguing that it “will force people into less controlled, private gatherings with no safety precautions – resulting in the exact opposite of slowing the spread” of the virus. The organization said that without being allowed to serve indoors in some capacity, “our state’s largest private sector employer will be pushed to the brink of permanent devastation.”
Mark Domitrovich, co-owner of Chicago restaurants Ina Mae Tavern and Frontier, said he was trying to “string together as much as an outdoor dining situation as we can get” because takeout and delivery alone weren’t enough to get by.
“At this point we’re trying to grind it out. To try to drive as much business as possible,” he said. “It’ll run out at some point and it doesn’t seem like the cavalry is on the way either, so we’re just praying right now.”
Pandemic Thanksgiving plans pivot after a surge in coronavirus cases
Health & BeautyNov 25. 2020Cat Lanigan, 23, and her roommates made the decision to take extra precautions, including not eating out, in preparation to travel to see their families at Thanksgiving. MUST CREDIT: Photo by Amanda Voisard for The Washington Post.
By The Washington Post · Emily Davies · NATIONAL, HEALTH, HEALTH-NEWS
Just two weeks ago, Dena Nihart finalized plans to meet dozens of relatives for Thanksgiving dinner beneath a tent in North Carolina’s Outer Banks. They agreed to quarantine for 14 days before the holiday and rent 10 tables so they could separate by household during the big meal.
But then, last Monday, Nihart’s body began to ache. By Wednesday, she could barely hold up her head. And by Friday, as Nihart waited for her coronavirus test results with cases surging around her, her family had canceled Thanksgiving altogether.
“It just sucks,” Nihart said from her bedroom, where she had just placed an online order for a turkey breast. The 45-year-old, who works for a construction company, will spend the holiday alone in her apartment in Arlington, Va.
Families across the region were willing to do almost anything to see one another for Thanksgiving this year. After a long and lonely summer, the number of coronavirus cases seemed to be just low enough by fall that it appeared as though they could find a way to safely gather for the holiday. The recent spike in community spread, however, has thrown a wrench into even the best laid plans. Newly sickened, exposed or fearing the rampant spread of the virus, people in D.C. and beyond say they are canceling their Thanksgiving plans and preparing for Turkey Day at home.
One area epidemiologist called off a trip to New Jersey a few weeks ago, and is now searching for a park at a halfway point to meet her family for a distanced tailgate. Another couple canceled their dinner reservations in an outdoor tent in favor of a carryout meal. Two roommates, 24 and 25, decided to have a wine night instead of traveling home to Texas. And a deacon whose pastor exposed him to the coronavirus last weekend is preparing for a quiet night alone.
The last-minute pivots are in line with new guidance from the Centers for Disease Control and Prevention, which on Thursday recommended against traveling or gathering for the holiday. Agency officials stressed that 1 million new cases were reported in the country in the week before Thanksgiving and warned that small gatherings of friends and relatives could accelerate the outbreak. Leaders in the Washington region echoed the guidance multiple times leading up to the holiday, pleading with their constituents to opt for virtual celebrations.
Still, many area residents are hoping to get together with loved ones be it outdoors or in small numbers. Thousands of people preparing to see relatives and friends lined up at coronavirus testing sites across the District over the past week. The number of people tested daily has risen from fewer than 2,000 during the summer to as many as 4,200, said Christopher Geldart, the city’s director of public works.
On Thursday, Cat Lanigan stood with her laptop in hand about halfway through a line that wrapped around five blocks from a coronavirus testing site in Northeast Washington.
Two weeks ago, Lanigan, 23, and her three roommates decided to condense their pod and stop eating at restaurants to prepare to go home for the holidays. They all were getting tested before traveling home to see older parents and family members.
“I feel like I just need to go home with people I can feel safe with,” she said. “I just feel so much instability right now. Covid changes. The political landscape changes. It’s mental health.”
Lanigan plans to drive home Tuesday to reunite with her immediate family of five, a far cry from her standard 40-person holiday gathering, but a comfort nonetheless.
Danielle Quarles, 41, a director of clinical research in Arlington, decided to abandon plans to see family near New York because of the rising number of coronavirus cases. Instead, she will drive her kids to meet up with their cousins at a park in Philadelphia if they all receive negative coronavirus tests.
“We know that winter is going to be hard and we won’t have opportunities to do it very often as covid continues to surge and the weather is cold,” she said. “So we really just wanted to find a way to let the kids see each other.”
The cousins plan to roam the park in masks and munch on pre-packed turkey.
Others faced with spending the holiday alone have turned to volunteer organizations to find community. Liana Ruiz, 22, who tutors a pod of students in Arlington, has only her cat, Yuki, left as Thanksgiving company after her parents forbade her from coming home because of coronavirus concerns.
She signed up for multiple shifts with Food & Friends, a local nonprofit organization that prepares and delivers meals to thousands of Washington-area residents.
Martha’s Table, a longtime D.C. charity, has more than 100 volunteers signed up for its annual Community Harvest Dinner. This year, the thousands of expected attendees will walk up or drive through to receive meals.
Only a few days away from Pandemic Thanksgiving, some locals are still deciding where, and with whom, they will spend the holiday.
Tyrus Williams, 24, stood at the end of a snaking line for a coronavirus test Thursday afternoon, his first trip out of the house since he received a positive diagnosis two weeks prior. His body aches were gone, congestion cured. But the test would help determine whether he could travel home for his favorite holiday.
Every year, Williams spends months looking forward to Thanksgiving, when many people gather at his family home in Massachusetts. This year, he hoped that at least a subset of the annual group would get tested and quarantine so they could get together for a big meal and hours of watching football on the couch.
“How am I feeling? I’m upset. This is my favorite holiday, and now it’s not going to be a thing,” Williams said before asking an emergency medical services professional near him whether enough tests were available that day (they were).
But it was not only Williams’s test that stood between him and a semi-normal Thanksgiving. On Wednesday, his mom began to feel sick.
“And she does all the cooking, so if she has covid,” he said, “no one is doing Thanksgiving.”
By The Washington Post · Lena H. Sun · NATIONAL, HEALTH, HEALTH-NEWS
WASHINGTON – The federal government plans to send 6.4 million doses of pharmaceutical giant Pfizer’s coronavirus vaccine to communities across the United States within 24 hours of regulatory clearance, with the expectation that shots will be administered quickly to front-line health-care workers, the top priority group, officials said Tuesday.
Gen. Gustave Perna, who oversees logistics for Operation Warp Speed, the Trump administration’s effort to speed up treatments and vaccines, told reporters that state officials were informed Friday night of the allocation, which is based on each state’s overall population.
The amount would cover a portion of the nation’s 20 million health-care workers, let alone the U.S. population of 330 million. But Perna said “a steady drumbeat” of additional doses will be delivered as manufacturing capacity ramps up in each successive week.
With increased prospects that federal regulators will authorize the Pfizer vaccine on an emergency basis as early as mid-December, and the first shots administered before the end of the year, Operation Warp Speed has begun to release more details about the massive and complicated distribution effort to immunize tens of millions of Americans.
U.S. government officials are on track to have 40 million doses of vaccines from Pfizer and a second company, biotech firm Moderna, by the end of the year, enough to vaccinate 20 million people. (Each vaccine requires two doses). It is likely to be April before the general public begins to get vaccinated.
The initial 6.4 million doses also includes vaccines that would go to five federal agencies – the Bureau of Prisons, the Defense and State departments, Indian Health Service, and the Veterans Health Administration – that receive allocations directly from the federal government.
States and territories now have the necessary information to “plan and figure out where they want the vaccine distributed” in the first shipment, Perna said. States are supposed to designate their top five sites capable of receiving and administering the Pfizer vaccine, which must be stored at ultracold temperatures of minus-70 Celsius (minus-94 Fahrenheit), and has exacting handling protocols. The ultracold temperature is significantly below the standard for most vaccines of 2-8 degrees Celsius (36-46°F).
Many states have designated large hospital systems to be the first places to receive vaccines because they have ultracold freezers and can efficiently vaccinate many people. The minimum order for the Pfizer vaccine is 975 doses; for Moderna’s, with a storage temperature that does not require such freezers, the minimum order is 100.
Once a vaccine is cleared by the FDA, an independent advisory panel to the Centers for Disease Control and Prevention – the Advisory Committee on Immunization Practices – will hold a public meeting within 48 hours to vote on final recommendations for the vaccine’s use and who should get the first shots. Health-care workers will be the first priority, the group has said. About 3 million residents of long-term care facilities are also likely to be included in that first phase. Next in line will be an estimated 87 million other essential workers, including first responders, teachers and grocery workers; more than 100 million adults with high-risk medical conditions; and about 53 million adults over the age of 65.
Within 24 hours of FDA action, doses will be “propositioned” at the sites designated by each state to give the shots to the first groups.
Pfizer has been conducting dry runs of each step, from vaccine delivery to opening Pfizer’s GPS-tracked special containers to vaccine storage, Perna said. The company began working last week with four states – Rhode Island, New Mexico, Tennessee and Texas – to familiarize personnel with storage and handling requirements. These dry runs do not include actual vaccines or the dry ice that will be used to keep the vials cold. Additional rehearsals in coming weeks will include dry ice, a federal health official said, speaking on the condition of anonymity because the person was not authorized to speak publicly.
Those “lessons learned” are being shared with other officials, Perna said. There was “initial hesitation” from some personnel at the sites, he said, but “we expect to see growing confidence in people that are using it.”
Americans will receive the vaccine free. The federal government is paying for much of the delivery and vaccine administration costs. But funding remains a big issue for state and local officials, who are asking Congress for at least $8 billion for vaccination efforts; to date, $200 million in federal funds has been sent to state, territorial and local jurisdictions to help them prepare. Federal officials are sending another $140 million in December.
Jeff Duchin, a top official at the Seattle and King County health department, said the more than $10 billion in taxpayer dollars spent on development of covid-19 vaccines by Operation Warp Speed was appropriate.
“But it’s been more like Operation Status Quo with respect to providing the federal funding needed for state and local health departments to actually get vaccine to the population, including the initial priority populations and ultimately, to as many people as possible,” he said in an email Tuesday.
State and local officials say much of the critical planning and implementation work needed for distribution is not adequately funded or staffed. That work includes planning with a broad range of health-care providers for the necessary training and upgrading information systems to vaccinate hard-to-reach and undeserved populations, Duchin said.
Health-care providers also need to track allocations and vaccinations administered, and ensure that people come back for second doses. Public health officials also need to do outreach with local communities that are hesitant about getting the vaccine, he said.
“Tens of millions of dollars are needed for this work in our county and state,” he said. “In addition, this work is tasked to local and state public health departments and workers, who have been grappling with this pandemic nonstop for months and are running on fumes.”
AstraZeneca coronavirus vaccine up to 90% effective and easily transportable, company says
Health & BeautyNov 24. 2020Suzanne Sunday participates in the AstraZeneca vaccine trial at NYU Langone Health in New York. MUST CREDIT: Photo by Sarah Blesener for The Washington Post.
By The Washington Post · William Booth, Carolyn Y. Johnson · NATIONAL, WORLD, HEALTH, HEALTH-NEWS
LONDON – AstraZeneca on Monday became the third pharmaceutical company to announce positive results from late-stage trials of a coronavirus vaccine, saying that its candidate, developed by Oxford University, is up to 90% effective.
The company is expected to fine-tune its vaccine trial in the United States in the coming weeks. MUST CREDIT: Photo by Sarah Blesener for The Washington Post.
Scientists and politicians alike hailed the third straight week of buoyant scientific news as a sign that, even as coronavirus cases surge to devastating levels in many countries, an end to the pandemic is in sight.
Pfizer and its German partner BioNTech and Moderna have each reported vaccines that were 95% effective in clinical trials. The AstraZeneca trial was 70% effective overall, with up to 90% efficacy in a smaller group that got a lower dosage. Different trial designs make direct comparison complicated, but even with somewhat lower protection, the AstraZeneca vaccine may be a more realistic option for much of the world, as it is likely to be less expensive and does not need to be stored at subzero temperatures.
Peter Piot, director of the London School of Hygiene & Tropical Medicine, who was instrumental in the battle against AIDS, said the positive results from three vaccine candidates cannot be overestimated.
He said that “2020 will be remembered for the many lives lost from covid-19, lockdowns and the U.S. election. Science should now be added to this list.” He added that “the only way to stop covid-19 in its tracks is having multiple effective and safe vaccines that can be deployed all around the world and in vast quantities.”
“I’m totally delighted,” said Hildegund C.J. Ertl, a vaccine expert at the Wistar Institute in Philadelphia. “What it tells me is this virus can be beaten quite easily: 90 to 95% efficacy is something we’d dream about for influenza virus, and we’d never get it.”
In years when the flu vaccine is a good match for the strain in circulation, it ranges between 40 and 60% effective.
The Oxford-AstraZeneca team said in a video conference with journalists that its candidate offered 90% protection against the coronavirus when a subject received half a dose, followed with a full dose one month later. Efficacy was lower – 62% – when subjects received two full doses a month apart.
Andrew Pollard, chief investigator of the Oxford trial, said the findings showed that the vaccine would save many lives.
“Excitingly, we’ve found that one of our dosing regimens may be around 90% effective, and if this dosing regimen is used, more people could be vaccinated with planned vaccine supply,” he said.
Britain has preordered 100 million doses – which at a dose and a half per person would cover most of its population. The United States has ordered 300 million, though both countries have hedged their bets and signed multiple vaccine deals.
The AstraZeneca results have yet to be peer-reviewed or published, and outside scientists said that much depended on seeing those in detail. Many questions remain, including why the lower-dose regimen was more effective. It is also unclear whether the vaccine can reduce transmission of the coronavirus by people who have no symptoms, which would have repercussions for how soon people could stop wearing masks. No one yet knows how long immunity from the vaccine will last.
Sarah Gilbert, a lead Oxford researcher, cautioned that the dose-and-a-half regimen would have to be studied more closely to be fully understood. But she said that the first half-dose might be priming a person’s immune system just enough, and that the booster would then encourage the body to produce a robust defense against infection.
AstraZeneca and Oxford have been conducting Phase 3 clinical trials worldwide, with the most recent data coming from an interim analysis based on 131 coronavirus infections in Britain and Brazil among nearly 23,000 volunteers, with half receiving the vaccine and half getting a placebo.
The company said it will present the results to Britain’s health-care products regulators immediately and will discuss its latest data with U.S. regulators as soon as possible. It is still only midway through its U.S. clinical trial, though, and now wants to adjust the format to further assess the half-dose shot plus booster.
But Michael Kinch, director of the Center for Research Innovation in Business at Washington University in St. Louis, said there needs to be more transparency about the findings. He said the reliance on foreign data, the lack of clarity about which dose should be considered by regulators, and the fact the trial found the stronger 90% efficacy in a small subset of people – fewer than 3,000 people received the dose-and-a-half regimen – raised concern.
“Under normal circumstances, I would say this would not be looked at favorably,” Kinch said.
World markets have rallied on optimistic vaccine news, although shares in AstraZeneca were down Monday on the London Stock Exchange.
Because the vaccine is in production, if approved, the first 4 million doses could be ready in December, and 40 million could be delivered in the first quarter of 2021, company executives said. By the spring, the company and its global partners in Brazil, India, Russia and the United States could be producing 100 million to 200 million doses a month.
At a news conference Monday evening, British Prime Minister Boris Johnson said, “With a favourable wind we should be able to inoculate the vast majority of the people who need the most protection by Easter.”
Johnson – who had the virus last spring and spent several days in an intensive care unit – told Parliament on Monday that vaccines are “edging ever closer to liberating us from the virus, demonstrating emphatically that this is not a pandemic without end.”
No participants who received the vaccine developed severe cases of the coronavirus or required hospitalization, AstraZeneca said Monday. The drugmaker also said that no “serious safety events” were reported in connection with the vaccine, which was typically “well tolerated” by participants regardless of their dosing levels or ages.
The vaccine uses a harmless cold virus that typically infects chimpanzees to deliver to the body’s cells the genetic code of the spike protein that dots the outside of the coronavirus. That teaches the body’s immune system to block the real virus.
Although the reason the regimen with an initial half-dose worked better remains unclear, Ertl said that it could be related to the fact that the body’s immune system can develop a defense mechanism to block the harmless virus that’s used to deliver the spike protein’s code. Giving a smaller initial dose may lessen those defenses, and make the vaccine more effective.
Several other vaccines in late-stage development use a similar technology, harnessing a harmless virus to deliver a payload that will teach the immune system how to fight off the real thing – including a Johnson & Johnson vaccine, a Russian vaccine being developed by the Gamaleya Research Institute and a vaccine made by CanSino Biologics in China.
The Pfizer and Moderna vaccines both use messenger RNA, a new vaccine platform never approved in a medical product for people.
Although the AstraZeneca results indicate somewhat lower efficacy, the vaccine can be stored and transported at normal refrigerated temperatures for up to six months. That could make it significantly easier to distribute around the world than Pfizer’s vaccine, which must be stored at minus-70 degrees Celsius, or Moderna’s, which is stable in refrigerated conditions for only 30 days and must be frozen at minus-20 degrees Celsius after that.
Gilbert and her team began developing the AstraZeneca vaccine in a small laboratory at Oxford on a shoestring budget. The university kicked in $1.3 million and then chose AstraZeneca as a manufacturing partner.
“We wanted to ensure there wouldn’t be any profiteering off the pandemic,” said Louise Richardson, the university’s vice chancellor, so that their vaccine would be widely distributed “and wouldn’t just be for the wealthy and the first world.”
The scientists said that although it appeared to be a race, or a competition, among the front-running vaccine developers, no one company could produce the millions of doses needed to end the pandemic.
“We don’t have enough supply for the whole planet,” Pollard said, adding that the important message is that there are at least three highly effective, safe vaccines that also appear to work well among the elderly, and that they are produced using different technologies, ensuring the quickest route to manufacture the billions of doses that will be needed.
Pollard said that it is “unclear why” the different vaccines were producing different results, and that he and the scientific community are awaiting full data from all the clinical trials. He said different studies were also using different end points to describe efficacy.
“At this moment, we can’t fully explain the differences,” Pollard said. “It’s critical to understand what everyone is measuring.”
Getting a coronavirus vaccine from loading dock to upper arm may be the hardest part
Health & BeautyNov 24. 2020Ahmed El Kority, pharmacy director at Riverside Shore Memorial Hospital in Virginia, inspects a new ultracold freezer that will be used to store coronavirus vaccine that must be kept as cold as minus-70 Celsius. MUST CREDIT: Photo for The Washington Post by Parker Michels-Boyce
By The Washington Post · Lena H. Sun, Frances Stead Sellers · NATIONAL, HEALTH, HEALTH-NEWS
Riverside Health System in Virginia has ordered a specialized freezer for each of its five hospitals to keep precious vials of coronavirus vaccine as cold as a deep Antarctic freeze.
Public health officials in Nashville and Baltimore are revamping routine flu clinics to test delivery methods for coronavirus vaccinations.
And in Maine, top health official Nirav Shah spends sleepless nights devising drive-through immunization facilities where vaccinators won’t have to wear winter parkas in addition to their personal protective gear.
Shah’s solution? Fire stations and carwashes.
Those venues are heated “so you have shelter from the snow and cold,” he said. “We haven’t inked any of those agreements yet, but that’s where our head is at.”
Buoyed by promising results from major clinical trials of three coronavirus vaccines, public health officials are preparing for the daunting task ahead of delivering those shots to tens of millions of Americans. On Monday, a third pharmaceutical company announced positive results from late-stage trials of a coronavirus vaccine, saying that its candidate is up to 90 percent effective.
The vaccines need to be distributed across 50 states, plus U.S. territories, that have different demographics and shifting needs. The leading products must be stored at different temperatures and have different minimum orders, with each requiring two shots but at different intervals.
Complicating matters: A final decision on who is eligible to get the early doses must wait for a federal advisory group’s recommendations. That can’t happen until regulators authorize the new vaccines. And once set in motion, the distribution – from loading dock to upper arm – has to be accomplished equitably and with as few handoffs as possible because it’s all being done amid a pandemic.
The stakes are enormous. The massive undertaking to immunize most of the population requires extraordinary communication, planning and coordination. Federal, state and local officials are working with hospitals and pharmacies, suppliers of dry ice, gloves and vials, and carriers such as UPS and FedEx. A successful operation could transform the health and economic well-being of society, in the United States and overseas.
“There are a million moving parts,” said Bruce Gellin, president of global immunization at the Sabin Vaccine Institute. “The system is complex to start with, [and] it is being modified to mount an immunization campaign of historic proportions,” he said, warning that while “expectations are sky high,” there are pitfalls at every step.
Officials are wrestling with how to ensure vulnerable populations receive the vaccine. Almost certainly at the front of the line: about 21 million front-line health-care workers. Next up are likely to be other essential workers, many of whom come from Black, Latino and Asian communities hard hit because of socioeconomic factors. Many can’t work from home, don’t have transportation and live in crowded housing.
“It’s like treating an individual patient while rebuilding the entire health-care system,” said Alfred Sommer, former dean of the Johns Hopkins Bloomberg School of Public Health, who was part of the team that vanquished smallpox four decades ago. Challenges will crop up, he said, such as immunizing disadvantaged communities. “Even with special outreach programs, it will not be easy with the vaccines ready for approval.”
Further complicating the logistics: the continued intrusion of politics. The Trump administration has not given information about vaccine distribution to the Biden transition team, President-elect Joe Biden’s chief of staff, Ron Klain, said in an interview Sunday on ABC’s “This Week,” adding to the potential for disruption.
“I have faith that the incoming administration will not completely upend the thousands of man and woman hours of work we’ve put in,” said Cindy Williams, vice president of the Riverside Health System and a member of Virginia’s coronavirus advisory committee. “Creating additional chaos as we’re managing this is really a bad idea.”
Once the vaccines are authorized by the Food and Drug Administration, doses will be allocated to each state according to population, with some held in reserve in case of loss or theft. Within 24 hours of FDA action, doses will be “prepositioned” at key sites designated by each state where vaccines will be administered to the first priority groups.
U.S. government officials anticipate having 40 million doses of vaccines from pharmaceutical giant Pfizer and biotech firm Moderna by the end of the year, enough to vaccinate 20 million people, a small fraction of the U.S. population of 330 million. (The United States will receive about half of Pfizer’s 50 million doses globally.) Government officials say it will be April before most people could get vaccinated.
The good news from AstraZeneca, manufacturer of the third vaccine, which is easier to store and transport, means the company will also apply for regulatory approval in the United States.
Americans will receive coronavirus vaccines free. The federal government is paying for much of the delivery and vaccine administration costs. But state officials are asking Congress for at least $8 billion for vaccination efforts; to date, $200 million in federal funds has been sent to state, territorial and local jurisdictions.
The vials will be sent first to large hospitals and other sites where mass immunization clinics can take place. But even that first step presents daunting travel, storage and handling requirements.
The Pfizer vaccine will be shipped to sites selected by states in GPS-tracked, suitcase-sized “shippers” with 50 pounds of dry ice pellets, and must be kept at minus-70 Celsius. Upon arrival, the dry ice must be refreshed, or the vials of vaccine must be transferred to ultralow-temperature freezers. The specifications are exacting if the vials stay in the shippers: The container cannot be opened more than twice a day, the dry ice must be replenished every five days, and the contents must be used within 15 days. The vials can stay at refrigerator temperature for five days before their contents degrade.
The Moderna vaccine is less demanding, with a storage temperature of minus-20 Celsius, which is the same for many medications.
The shipments need to be coordinated with kits of syringes, needles, face masks and other ancillary supplies.
From there, every state, territory and each of six major metropolitan areas is responsible for its own deployments. States are in varying stages of preparation. Many have designated large hospital systems to be the first places to receive vaccine. Maine, for example, has chosen five hospitals with ultracold freezers to receive its first doses, and each has a plan to reach into the community. But just in case, the state bought an ultracold freezer for its public health emergency warehouse that can store more than 200,000 doses.
Maine has held meetings with transportation officials and the National Guard to work through worst-case scenarios, Shah said. If there’s a flood or loss of power, a backup generator for the freezer would kick in. If shots are transported during a blizzard, the vaccine convoy could follow 30 minutes behind a salt truck.
The Centers for Disease Control and Prevention has told states they don’t need to buy specialized freezers because immunizations in the earliest phases will focus on sites that can vaccinate as many people as possible and will be able to handle the cold chain requirements, even without freezers.
But at the Henry Ford Health System in Detroit, Northwell Health in New York and Riverside in Virginia, officials bought them anyway, executives said on a conference call Thursday about vaccine distribution organized by Premier, the group purchasing organization and supply consultancy for 4,100 hospitals. The executives’ assumption was that early public vaccination clinics will be most efficiently done on the campuses of hospitals with ultracold freezers.
Among them is Riverside Shore Memorial Hospital on Virginia’s Eastern Shore, a medically underserved and rural community that includes poultry and agricultural workers who did not have health insurance until the state recently expanded Medicaid, said Williams, of Riverside Health. It is one of three major health-care providers for the community, and the only one with an ultracold freezer.
Clinicians will need to be trained to administer the vaccines, which have different protocols. The Pfizer version must be diluted before the shot is given – inverting the vial 10 times “gently,” according to the Pfizer instructions. In contrast, the Moderna vaccine does not require on-site mixing and should not be shaken.
To start with, vaccination efforts may favor urban areas. That’s because the vaccines will arrive in big batches: For Pfizer, the minimum order is 975 doses. Moderna’s smallest batch is 100 doses.
In Alaska, “you’re not going to have 900 people within 1,000 square miles,” said Danny Staley, a senior vice president at the Association of State and Territorial Health Officials. “You’re wanting to do that at a mass vaccination clinic, where we know people can use it so we don’t waste it,” he said.
“The most disadvantaging issue is the minimum order,” said Ann Lewandowski, program manager for the Southern Wisconsin Immunization Consortium, a group of 42 rural hospitals in Wisconsin. None has the resources to purchase a special freezer, which can cost $12,000 to $15,000 and might be needed for only a year until vaccines are developed that don’t require such frigid temperatures.
Identifying enough health-care workers to be immunized is also challenging for rural hospitals that may have only 20 nurses and 20 doctors. “You would need to reach out to pharmacists, reach out to dentists and all these other professionals, but 975 is really an impossible goal,” Lewandowski said.
On a recent call, a Pfizer representative told Lewandowski the company hopes to send out smaller batches of 125 doses by April. But even that creates logistical challenges because the vials need to be coordinated with the ancillary kits, which are equipped for 100 doses.
Health-care personnel from rural hospitals may have to drive to get their shots at larger hubs in Madison, Milwaukee or Eau Claire, Lewandowski said. That could pose a barrier for staffers already stretched thin caring for patients with covid-19, the illness caused by the coronavirus.
“These are health-care workers who are taking risks to serve the state in our time of need, and it’s not fair to discriminate against them simply because they live in a geographically challenged place,” Lewandowski said.
A Pfizer spokeswoman said the company is working on a smaller pack size that will be ready the first three months of 2021.
Final recommendations on who gets the first shots will come from an independent committee on immunizations that advises the CDC. There is broad agreement that health-care workers will be first, and will include clinicians, custodial staff, home health aides, pharmacists, paramedics and staff in long-term care facilities, according to meetings of the Advisory Committee on Immunization Practices. That first group may also include about three million long-term care residents.
Jose Romero, a pediatric infectious-diseases specialist who chairs the immunization panel, said “essential workers” are likely to be high on the list. That might include people who stock supermarket shelves or pick vegetables, many of whom belong to communities of color devastated by covid-19.
“That is part of the equity question we are trying to solve,” Romero said.
That assumes priority groups are willing to take the first shots. Health officials say they are increasingly worried about staffers who say they won’t take the vaccine, according to internal surveys and conversations with clinicians.
“When it comes to this vaccine, what I’m hearing from colleagues . . . is that their confidence is lacking,” Pamela G. Rockwell, a physician representing the American Academy of Family Physicians, said during last month’s meeting of the federal immunization advisory committee.
“I’m already won over,” she said. “We need to win over a lot of primary care physicians . . . We need to do this right and get our patients convinced that this is safe so we can save our country.”
Federal health officials are also concerned.
“I am worried that people are going to equate the complicated storage and handling as somehow more reason to be hesitant about the vaccine, when in fact, it has nothing to do with how well the vaccines work,” said a senior federal health official involved in distribution with the Defense Department and private industry. The official spoke on the condition of anonymity because they were not authorized to speak publicly on the record.
At Riverside, a survey last month of about 1,000 employees, most in nursing and administrative positions, found about a third said they would take the vaccine, another third said they would not, and the remainder wanted more data on safety and efficacy. A separate poll of physicians found nearly half would not take the vaccine. The surveys were conducted before reports about the vaccines’ effectiveness, and acceptance is likely to increase, said Riverside’s Williams.
Patients will be more likely to be vaccinated if they ask their doctors if they’re willing to be vaccinated and the physician says yes, she said.
Saad B. Omer, an epidemiologist and infectious-diseases expert who directs the Yale Institute for Global Health, has done extensive studies about the political and social factors influencing trust in vaccines. What he sees now is not “your run-of-the-mill vaccine hesitancy.” President Donald Trump’s actions fueled mistrust in science, he said.
But health-care personnel can be persuaded. Strong endorsements from a trusted person, such as Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, can make a huge difference, according to a study Omer conducted recently.
Experts who study vaccine hesitancy say promotional campaigns that use social media and increase community engagement with trusted leaders will be key to encouraging use of a new vaccine.
Adam Abadir, director of communications at the Baltimore City Health Department, said the city’s health officials had been using routine flu clinics to hone strategies such as tailored social media campaigns and outreach through pastors and other trusted community members.
“We now have partners in place who can deliver the messages,” Abadir said, even though he doesn’t yet know what those messages will say.
In Nashville, the annual “Flulapalooza” mass vaccination event at Vanderbilt University Medical Center – last year, they managed 15,000 shots on site in one day – was modified as Flula-2-uza to test strategies for the coronavirus, which may involve reversing their strategy and venturing out to remote workers.
The new vaccines are likely to produce more unpleasant side-effects than a flu shot, potentially leading recipients to need a day or two off work.
“Any group of individuals that work together, we can’t vaccinate them all at the same time,” said Thomas Talbot, chief hospital epidemiologist at Vanderbilt, which will likely be among the first sites to receive the Pfizer vaccine and is looking at how to stagger immunizations to minimize the impact on departments.
In Baltimore, a mobile flu clinic in a predominantly Latino community drew more than 150 people on a recent stormy morning to a school parking lot, where a team of Spanish-speaking officials were working with next year in mind.
Drive-through vaccination isn’t viable for people in the city who lack transportation, said Rebecca Dineen, assistant commissioner for the city’s Bureau of Maternal and Child Health. So the health department is pushing hard to foster links in public housing and with neighborhood leaders who will be key to coronavirus distribution.
“You don’t need a fancy innovative approach,” Dineen said. “A lot of it is really knowing your people.”
Shah, in Maine, is hoping that beyond cultivating relationships with pharmacies and physicians offices, fire stations and carwashes will be all the innovation he needs.
“We think the fire departments are a pretty good source for sites because there are so many, many small towns in Maine,” he said.
EMS clinicians can be vaccinators there or at carwashes.
“People trust them,” he said. “And trust matters a lot.”
Smallest health providers face biggest problem finding protective gear
Health & BeautyNov 23. 2020Denadlhy Belleus Pierre puts on her equipment before helping patients with covid-19 antibody tests in Washington in June 2020. MUST CREDIT: Photo for The Washington Post by Amanda Voisard
By The Washington Post · Amy Goldstein · NATIONAL, HEALTH, HEALTH-NEWS
WASHINGTON – As the coronavirus rages across the country, community health centers and small doctors’ offices, AIDS clinics and homeless shelters are struggling with a scarcity of protective gear to buffer workers from harm, their budgets and buying power unable to compete with large medical institutions.
Most U.S. hospitals and health systems have, over the pandemic’s nine months, stitched together systems and improvisations to acquire masks, gowns, gloves and other personal protective equipment (PPE). Yet many small health-care and social-service settings continue to suffer from shortages they expect to grow worse.
A New Orleans mission for the homeless and addicted finally gave up searching for masks after an offer from a local sports team fizzled, so its staff members rely on disinfecting throughout the day. To conserve gowns, a Boston health center requires nurses to stand without them on the opposite side of plexiglass barriers from most patients who come for coronavirus tests, instructing people how to swab their own noses. And a pediatrician near Fredericksburg, Va., was thrilled when her husband spotted N95 masks at a nearby Lowe’s, because her office manager was unable to get more than a list of where to look for supplies from the state.
The scrounging and adapting to scarcity attest to a two-tier reality that has emerged in health workers’ ability to obtain the equipment that provides a physical barrier against the virus that has sickened more than 12 million people in the United States and killed at least 255,000.
“No one is talking about this huge inequity of availability,” said Megan Ranney, a Providence, R.I., emergency room doctor and Brown University researcher who in March co-founded with several other worried physicians Get Us PPE, a group that collects and distributes donated supplies.
Since it started, Get Us PPE has fulfilled 12% of the requests it has received – a percentage dropping lately as the pandemic intensifies and the eagerness for protective equipment increasingly outstrips donations. Yet requests from hospitals have declined from the thousands in April to fewer than 100 per month more recently, the group’s information shows.
This disparity – with small facilities facing PPE shortages to a greater extent than larger ones – has not been recognized in federal officials’ recent statements about masks, gloves, goggles and gowns to protect workers especially vulnerable to infection.
In a statement on the pandemic this month, President-elect Joe Biden said the government must provide “frontline health-care workers” with resources “including personal protective equipment that is again in short supply.” Nor did Senate Minority Leader Chuck Schumer, D-N.Y., and two other Senate Democrats draw the distinction among facilities last week when they announced a bill that would devote $10 billion to the federal Strategic National Stockpile to increase purchases of N95 masks and other protective supplies.
And in a briefing Thursday by the White House’s coronavirus task force, David Sanford, on loan from the Defense Department to the Federal Emergency Management Agency to oversee supplies, said: “Since the late summer, we have grown our personal protective equipment capability 10 times to 15 times” in the stockpile and at FEMA over levels before the pandemic, with four months’ worth of N95 masks likely to be needed in the current surge of cases. Sanford did not mention that some places still have trouble getting them.
According to hospital CEOs, state officials, procurement specialists and nonprofits such as Get Us PPE, shortages linger in some small hospitals, especially those in rural areas and the most intense virus hot spots.
Exam gloves are in a global shortage now, and some distributors of other supplies are rationing orders as the pandemic worsens and hospitalizations rise, according to David Gillan, senior vice president for sourcing at Vizient, a company that works with 60% of the nation’s hospitals on group purchasing and other performance improvements.
And many hospitals are getting by, using new government-approved protocols for cleaning and reusing N95 masks that were meant to be worn once and discarded.
At York General Hospital, with 25 beds in a small Nebraska town of that name, the hospital board voted to spend nearly $80,000 from its strained budget to buy a robot that disinfects with ultraviolet light to allow N95 masks to be used five times. The cleaning process meets guidelines issued this year by the Centers for Disease Control and Prevention. But Jennifer Uffelman, York General’s environmental health safety and security coordinator, said the hospital would “absolutely not” be reusing masks if it had an adequate supply.
“It just makes people feel better when they know they can go to the cupboard and get a new one,” Uffelman said. “It just makes people feel better to know we have the stock, we are not worried about shortages. But they know we are doing everything we can. . . . The science has said this is safe.”
Still, unlike in the pandemic’s early days, York now has a “burn rate calculator” the state handed out to track the use of PPE. And Doug Carlson, Nebraska’s chief procurement officer, said that, in late April, he and others created a model in which hospitals and other facilities fill out a form to submit to the state’s regional health districts and, once a week, supplies are distributed from a central warehouse.
Such systems were not common at the pandemic’s outset, and many hospitals – especially small ones – began relying on folkways they developed.
The Texas Organization of Rural and Community Hospitals had never bought members any type of supplies until its president, John Henderson, started getting frantic daily calls about PPE from many of the state’s 157 rural hospitals. “We were at the end of the supply chain, and the supply chain was broken,” he said.
TORCH, as the group is known, began developing relationships with vendors and buying and collecting donations of masks, hand sanitizer and other gear. It crammed boxes into its Austin offices and created chains of volunteers to drive, relay-style, across Texas’s expanse for deliveries.
Now, as the pandemic surges in West Texas, stressors are reemerging, and gloves are a particular trouble spot, Henderson said. But most of the state’s rural hospitals are far closer to having what they need, according to Henderson and several hospital chief executives.
In some corners of the nation, the scrounging has been even more homespun. At Mat-Su Regional Medical Center in Palmer, Alaska, nearly 40 miles north of Anchorage, Thomas Quimby, the emergency department’s medical director, became the leader of the hospital’s coronavirus task force in March.
“We were short on everything,” Quimby recalled. “We went around and bought up all the industrial respirators” the hospital could find and turned to a local distillery to start making hand sanitizer. But it could not find disposable gowns, so the task force came up with the idea of asking a local sewing club to make cloth versions.
One April day, Quimby reached for a gown among several hanging from an IV pole in the emergency department’s hallway – and realized that the cream-colored fabric printed with cowboys had been his favorite sheets as a boy. He had known that his mother, Sandy Quimby, a half-hour away in Eagle River, was a pack rat. He had not known that she was part of the Mat-Su Valley Makers, the sewing club.
Over several months, the hospital has phased out community-made gowns because it found a commercial supplier.
“I feel much better about PPE than when the first wave hit,” said Anne Zink, Alaska’s chief medical officer. Even though Alaska’s small population and great distance are hindrances to purchasing, she said, the state has been able to stockpile most of the equipment it needs for the hospitals it supplies.
Gillan, of Vizient, said hospitals in general have become less reliant on federal and state supplies because they have found ways to buy their own.
Despite the current glove shortage, Gillan said, “it’s remarkable to see how all of these hospitals are working with the manufacturers and the distributors.” And as a backup, he said, Vizient has built up its disaster response so that, when its client hospitals run low on certain PPE, “we address them when we’re made aware of those, one hospital at a time.”
Such buying power and reserve sources are far different than in the world that Steven Chies inhabits as president of North Cities Health Care, a family-owned company outside Minneapolis that runs two nursing homes and an assisted-living facility.
Large nursing facilities are faring better. But the most recent figures the American Health Care Association, a trade group, submitted to federal health officials on behalf of about 14,000 nursing homes, show that more than 600 were out of N95 masks and that an additional 900 or so had less than a one-week supply. Few are completely without gloves or gowns, the data indicates.
Yet as a small company without much buying clout, Chies said, “it’s week-to-week. It’s more of a gut punch when you don’t get what you ordered, and you’re concerned our staff won’t have the right equipment. It’s just scary at that point.” This month, all of the suppliers he relies on have cut back on what they are willing to send, and Chies fears scarcity will grow as coronavirus cases keep setting records.
At the moment, his workers have enough gloves and surgical masks, but supplies of disposable gowns are low, and N95 masks are so scarce that workers use them only when entering the rooms of patients with nebulizers for asthma or other equipment that increases the spread of aerosols.
That sense of relative scarcity is familiar to Genevieve Daftary, director of pediatric medicine at Codman Square Health Center in Boston, in the shadow of the city’s large, well-heeled academic medical centers. Protective equipment “is not a budget item for an organization always operating on the margin,” she said. “What we’ve realized is there is no cavalry coming,” despite an intense effort by the development staff to raise money for such supplies and find donations.
“We’ve learned to triage, not just the patients, but triage the PPE,” Daftary said.
Of 2,900 face shields on hand, fewer than one-third have padding at the forehead and comfortable elastic at the back. The rest, less expensive, “are the ones giving you a headache” by the end of the day, she said.
Over the months, the health center has altered protocols so that fewer workers need to wear the scarce gowns and masks. Patients arriving for a test with the worst symptoms typical of covid-19, the illness caused by the novel coronavirus, are ushered into an exam room in the clinic’s urgent-care section. Just outside the room, a nurse practitioner, physician assistant or doctor – not suited up in protective gear – calls the patient, who picks up a phone on the room’s desk, and the medical worker takes the patient history. Only after getting filled in does another staff member wearing protective gear duck inside to see the patient, limiting exposure, while wearing the same gown all day.
People without symptoms, or with mild ones, are directed for tests to an auditorium down the street, where they are seated before tables with laminated instructions, tissues, a swab and a vial. A three-sided plexiglass wall separates them from a clinic staff member, stationed at least six feet away – using a face shield but no mask – to talk them through the test.
In Spotsylvania, Va., Suzanne Richman, a pediatrician in solo practice, began trying to order gowns last winter from McKesson, a major health-care supplier. It was August before a box of 50 arrived, she said.
At one point in the spring, Richman asked her office manager to check with the regional arm of the Virginia Department of Emergency Management, which helps provide PPE. What arrived at Richman’s office was a list of companies to check with about supplies – including McKesson, which wasn’t sending her any.
But, she said, “we were lucky.” One spring day, her husband happened to be at a Lowe’s home improvement center and called to say the store had a couple of boxes of N95 masks. “Buy them all,” she told him.
The New Orleans Mission has stopped looking for masks. It has three sites and provides shelter. It offers addiction treatment and job training to about 300 people at a time.
“We can’t get it, and we can’t afford it,” David Bottner, the mission’s chief executive, said of PPE. New Orleans was an early pandemic hot spot, and Bottner’s staff searched hard for protective gear, looking for donors or help from city government. Finally, as the season’s first hurricane threatened, the city sent a box of masks. It contained 50, enough to last the staff less than two days.
Now, the mission gives out a mask only when people ask. But cleaning five times a day, with a strict rule about temperature checks before anyone enters, has held coronavirus cases over the months to 17 among clients and two among workers.
In September, a representative of a sports team called, Bottner said. “They had a coach that was setting up a fund to buy PPE to help facilities like ours,” Bottner said he was told.

 On the road outside rural Wessington Springs, S.D., where 1 in 37 people had the virus this month. MUST CREDIT: Photo for The Washington Post by Jenn Ackerman
On the road outside rural Wessington Springs, S.D., where 1 in 37 people had the virus this month. MUST CREDIT: Photo for The Washington Post by Jenn Ackerman 

 Cat Lanigan, 23, and her roommates made the decision to take extra precautions, including not eating out, in preparation to travel to see their families at Thanksgiving. MUST CREDIT: Photo by Amanda Voisard for The Washington Post.
Cat Lanigan, 23, and her roommates made the decision to take extra precautions, including not eating out, in preparation to travel to see their families at Thanksgiving. MUST CREDIT: Photo by Amanda Voisard for The Washington Post. 
 Suzanne Sunday participates in the AstraZeneca vaccine trial at NYU Langone Health in New York. MUST CREDIT: Photo by Sarah Blesener for The Washington Post.
Suzanne Sunday participates in the AstraZeneca vaccine trial at NYU Langone Health in New York. MUST CREDIT: Photo by Sarah Blesener for The Washington Post. 
 Ahmed El Kority, pharmacy director at Riverside Shore Memorial Hospital in Virginia, inspects a new ultracold freezer that will be used to store coronavirus vaccine that must be kept as cold as minus-70 Celsius. MUST CREDIT: Photo for The Washington Post by Parker Michels-Boyce
Ahmed El Kority, pharmacy director at Riverside Shore Memorial Hospital in Virginia, inspects a new ultracold freezer that will be used to store coronavirus vaccine that must be kept as cold as minus-70 Celsius. MUST CREDIT: Photo for The Washington Post by Parker Michels-Boyce 
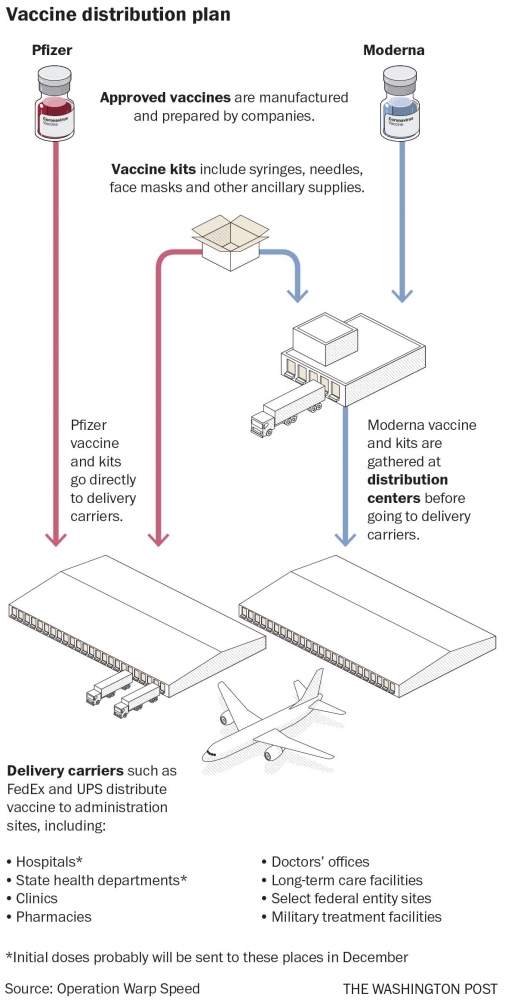
 Denadlhy Belleus Pierre puts on her equipment before helping patients with covid-19 antibody tests in Washington in June 2020. MUST CREDIT: Photo for The Washington Post by Amanda Voisard
Denadlhy Belleus Pierre puts on her equipment before helping patients with covid-19 antibody tests in Washington in June 2020. MUST CREDIT: Photo for The Washington Post by Amanda Voisard 
