Covid-19 death rates are lower worldwide, but no one is sure whether that’s a blip or a trend
Health & BeautyOct 09. 2020Physician Peter Chang tracks coronavirus indicators, including hot spots in Tampa, where he works at Tampa General Hospital. MUST CREDIT: Washington Post photo by Michael S. Williamson.
By The Washington Post · Ariana Eunjung Cha, Loveday Morris, Michael Birnbaum · WORLD, HEALTH, HEALTH-NEWS After working for three months straight at Detroit Medical Center, Said El Zein noticed that the coronavirus patients who began arriving in May appeared less sick than those who came before.
More than 4,000 miles away in northern Italy, researcher Chiara Piubelli was struck by the same thing.
Rafael Cantón, an infectious-disease specialist in Madrid, also marveled at the change. “It’s totally different,” he said last month of the falling admissions at his medical center, noting that only 130 of 1,000 beds were full despite surging infections – a huge change from early spring when every bed was occupied.
Mortality decline Photo by: The Washington Post — The Washington Post
Death rates from the novel coronavirus are lower in hot spots around the world, even as new infections accelerate in what may be the pandemic’s next wave. Scientists are confident the change is real, but the reasons for it – and whether it will last – are a matter of intense debate.
“Is this a trend or a blip?” asked Joshua Barocas, an infectious-disease specialist at the Boston University School of Medicine. “Nobody really knows.”
The mortality rate of the coronavirus has been a moving target since the outbreak began.
Early reports out of China put it as high as 7%. But that was based mostly on hospitalized patients, and by the time the wave hit the United States, epidemiologists believed it was closer to 2 to 3%. Now, factoring in asymptomatic infections, as well as mild cases that might not be part of official tallies, the Centers for Disease Control and Prevention puts the mortality rate at 0.65%.
Rate Photo by: The Washington Post — The Washington Post
Barocas emphasized that even the lowest estimates represent the potential for millions more deaths. The United States already has the highest number of cases in the world and the most recorded deaths of any country. Though its 330 million people represent roughly 4.25% of the world’s population, the country has recorded just over 20% of deaths from covid-19, the disease caused by the coronavirus.
As we enter a new phase of the pandemic, Barocas said, with much of the country experiencing colder weather amid a reopening of more workplaces and schools, it’s too soon to be confident that mortality rates won’t tick up alongside case counts, as young people spread the disease to their elders.
He called this time “a cliffhanger moment.”
Public health officials cite multiple reasons for the lower death rates: They note a shift in the demographics of who is being stricken with the virus, with younger people making up the bulk of new infections. More widespread testing is capturing a more diverse range of people and illness, and improved treatment strategies that include antivirals and steroids are saving more lives.
But some researchers speculate there may be more to the story.
One prominent but still unproven theory suggested by early research is that we miscalculated humanity’s susceptibility to the coronavirus, and that a slice of the population may be partially immune, perhaps due to previous exposure to the common cold coronavirus, childhood vaccinations or something else.
The other possibility is that something important has changed in our environment – the weather, behaviors or the virus itself.
Most viruses lose their killing edge eventually, due to a lack of hosts, mutations that make them less deadly, or new treatments or vaccines. The novel coronavirus will, too, experts say, but it’s a matter of when and how many lives are lost until then. But most scientists doubt that’s what we are seeing now, based on genetic sequencing research.
One idea that has generated a lot of discussion recently, bolstered by two back-to-back studies – El Zein’s and another from Italy, presented in late September to the European Society of Clinical Microbiology and Infectious Diseases – is that social distancing and masks are reducing the dose of virus people are receiving, resulting in less-severe illness.
As El Zein and other doctors in Detroit probed why their patients appeared to be less ill, they were startled to find that one indicator in particular changed dramatically over time: viral load.
Among 708 patients treated by early summer, the average viral load – a measure of the particles of virus in the body as measured by nasal swabs – fell almost on a weekly basis. In most infectious diseases, including Ebola, HIV/AIDS and hepatitis, the higher the load, the worse the outcome.
El Zein saw glimmers of hope in the findings: Could it be that the steps being taken to mitigate the coronavirus’s effects were showing success?
Monica Gandhi, an infectious-diseases researcher at the University of California at San Francisco, shares that view. If the initial viral dose – known as the “inoculum” – is lower, she theorized, people’s bodies are able to fight back more effectively.
This “likely indicates an ability to control the viral infection better, and, therefore, have less severe disease,” Gandhi said.
– – –
Of the many mysteries of the coronavirus, perhaps the most important to the average person is his or her risk of death. For smallpox, it’s about 10%, thanks to treatments. For Ebola, it’s about 50%. For rabies, it’s almost 100%, making it the most lethal infectious disease on the planet.
President Donald Trump has repeatedly talked about coronavirus mortality rates, even claiming on Fox News in July that the United States had the “number-one low-mortality rate.” Those claims are incorrect, according to the White House’s own data (fact-checkers pointed out that the chart he was looking at that day was upside down). But the confusion underscores how complex the subject is and how such rates can vary dramatically over time, country, region, age and other factors.
“What you are seeing is a misapplication of data and statistics that ends up being overtly false and sometimes very, very misleading,” explained Amesh Adalja, a senior scholar at the Johns Hopkins Center for Health Security.
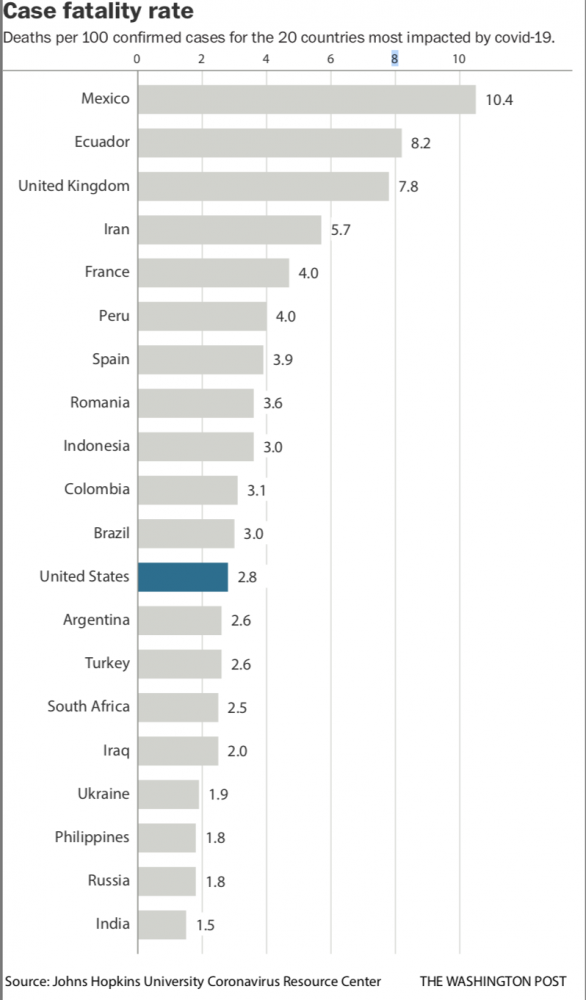
There are many different ways to measure deaths. The most-cited numbers – the ones often released by hospitals – are case fatality rates, or the percentage of deaths among confirmed cases. In contrast, the infection fatality rate is typically an estimate of deaths as a proportion of all those believed to be infected, including people who are asymptomatic or who have mild cases and may not have bothered to get tested, so they would not be counted as part of official tallies. So the former number often looks scarier than the latter.
According to a Johns Hopkins University analysis, which is updated daily, the case fatality rate in the United States was 2.8% as of Thursday. That compares with the CDC’s 0.65% estimated infection fatality rate – which includes confirmed cases plus an estimate of those who may not even know they have been exposed. The case fatality rate in the United States is much higher than in South Korea, Taiwan and Iceland, where it has been below 2%, but lower than in some other hard-hit countries, such as Iran and Brazil.
Some public health officials suggest part of the change in mortality rates is partly a mathematical trick: The more people we test, the larger the denominator of positive cases and the lower the mortality rate.
At the peak of Spain’s epidemic earlier this year, for example, Cantón said, he was doing 500 PCR tests a day, but now it’s more than five times that.
“It looks like we have more positive patients now,” said Cantón. “But this is because we are doing more diagnosis.”
Rinesh Parmar, an intensive care doctor who heads the United Kingdom’s Doctors’ Association, agreed: “The amount in the community was grossly underestimated. We were undertesting.”
Epidemiologists also look closely at deaths per 100,000 people in the population. Because that rate is less dependent on the wild variations in testing capacity, it can be a useful number to compare regions or nations.
To put these numbers into context, the infection fatality rate for the flu, Adalja said, is about 0.1%, making the coronavirus about six times more deadly.
“I think people don’t realize a small percentage of a big number is still a very big number,” he said. Sixty-five hundredths of the U.S. population of roughly 330 million, he pointed out, is 2.145 million – or 2.145 million potential deaths.
– – –
The earliest reports of a less-deadly coronavirus came on May 31 and drew widespread skepticism. Alberto Zangrillo, head of the San Raffaele Hospital in Milan in the northern region of Lombardy, which had been the epicenter of Italy’s outbreak, and Matteo Bassetti, from a hospital in Genoa, conjectured that the virus was weakening.
Zangrillo provided the first evidence that viral loads might be linked, stating that in the previous 10 days, nasal swabs taken at his hospital in Milan detected “absolutely infinitesimal” amounts of the virus as compared with the previous two months.
The claims were quickly denounced by public health officials who said there was no evidence of any change in the virus’s lethality. But over time, to some scientists’ surprise, the data has borne out the falling mortality rates and decreased viral load.
An Aug. 13 letter published in JAMA by doctors at Houston Methodist, which operates eight hospitals, reported huge differences between what they called surge 1 and surge 2 patients. In surge 2, which took place from May 16 to July 7, a smaller proportion of patients required intensive care (20%), as compared with those seen earlier, from March 13 to May 15, during surge 1 (38%). They spent less time in the hospital (4.8 days versus 7.1 days).
Most importantly, the later patients were much less likely to die – 5.1% versus 12.1%.
A broad analysis of 53 countries and regions with the highest coronavirus death rates identified similar trends. Published in September in Transboundary and Emerging Diseases by a group of American and Chinese researchers, the report found that 80% of countries and regions estimated lower case fatality rates in the disease’s second wave. The paper cited numerous possibilities for what might be driving the shift, including that the most vulnerable had already been infected and died in the first wave. Other theories involved better preparedness, the younger ages of those infected and more favorable environmental conditions, including warmer weather.
“Current evidence remains limited to suggest which of the above hypotheses is more plausible,” the authors wrote. However, they said the classical epidemiological triangle model, which states that “the interactions of the host, pathogen and environment determine the characteristics of outbreaks, rather than one or two factors alone,” likely holds true for the coronavirus.
Viral loads have been one of the most mystifying aspects of the virus.
The now widely available nasal swabs, or PCR tests, give a simple binary yes or no answer about the presence of the virus. But scientists have recently made new discoveries about the importance of the quantity of virus people carry.
When it comes to infectivity, scientists generally believe a negative PCR test, which indicates what is basically a viral load of zero, means you can’t transmit it. This is why the CDC originally recommended two negative tests 72 hours apart before people came out of self-isolation. A high viral load, on the other hand, is believed to mean higher infectivity.
There’s less certainty about how viral load relates to the patient’s own clinical course. Previous studies on influenza tell us that higher viral loads in hospitalized patients are generally not associated with worse outcomes. In contrast, for patients with MERS or SARS – the other severe coronaviruses – higher viral load was an independent risk factor for mortality.
The new Italian viral load study seems to support that link for the novel coronavirus, too. It found that in 373 patients seen in the emergency room in the city of Negrar in northern Italy, viral load declined from March through May, corresponding with a sharp drop in intensive care admissions over those months, down to zero in May.
In a presentation to other scientists in Europe last month, Piubelli, a researcher at Sacro Cuore-Don Calabria Hospital, surmised that “lockdown measures had an impact not only in the absolute number of infected people but also on the severity of clinical manifestations.”
El Zein’s study found more direct evidence that high viral load appears correlated with increased mortality. But the findings are considered preliminary because the team is still analyzing possible confounding factors, such as differing treatments, to see if the relationship holds. In the first week of the study, about 25% of the viral loads were high, half were intermediate and 25% were low. By the fifth week, about 12% had high viral loads, and in the sixth week, no patients had high viral loads.
The death rate of patients in the high viral load group was 45%, compared with 32% of those in the intermediate group and 14% in the low group.
El Zein said the relationship was so striking that he went back to the lab to check, double-check and then triple-check equipment, and to try to figure out whether anything had changed with the procedures for collecting samples, but found no differences.
“It definitely wasn’t by chance or by mistake those numbers are going down,” he said.
One puzzling thing, he noted, is that some studies have shown that children with high viral loads appear to be completely asymptomatic, although those levels correlate with those of adults in intensive care. Separately, the new coronavirus mutation becoming dominant in the world has been associated with higher viral loads in at least one study. El Zein has been stumped about how to reconcile that with his analysis and others of lower viral loads among recent patients.
As cases, hospitalizations and deaths in the United States and Europe have ticked upward in recent weeks – albeit with a lower proportion of deaths than in the past – some health officials have expressed concern that they will be overwhelmed by a slower but more sustained second wave. If the virus spreads back to older people, as many fear is inevitable, death rates may rocket back upward.
Even in Germany, considered a model for coronavirus control and which stood out this spring as an anomaly with a low case fatality rate of less than 0.5%, Health Minister Jens Spahn warned the rate would likely rise. Already, there are 470 patients in intensive care, double the number of a month ago, he said.
“People think that the virus isn’t as serious because we got through the summer well,” he said. “But that’s a false conclusion. It was because we took preventive measures that we did well.”
Spahn blamed the increase on a lax attitude among the younger population that “want to party, to travel, and think of themselves as invulnerable.”
Across the rest of the world, alarmed governments are scrambling to bring back restrictions that haven’t been in place since spring: Paris has closed its bars, Madrid has ordered residents not to leave the city, and Moscow has told companies to make sure at least 30% of their employees are working remotely starting next week.
In New York on Tuesday, about 100 public schools were ordered closed in neighborhoods that have seen a resurgence of the virus.
“It’s a matter of time before we see a rise,” said Steven Van Gucht, the head of viral diseases at Sciensano, Belgium’s national public health institute. “The characteristics of the virus have not changed.”
Contacts of Trump event guests may never be traced
Health & BeautyOct 09. 2020People listen as President Trump announces Judge Amy Coney Barrett as his nominee to the Supreme Court in the Rose Garden on Sept. 26. MUST CREDIT: Washington Post photo by Jabin Botsford
By The Washington Post · Isaac Stanley-Becker, Rosalind S. Helderman, Josh Dawsey, Amy Gardner · NATIONAL, HEALTH, POLITICS, SCIENCE-ENVIRONMENT WASHINGTON – An evangelical pastor preached in Georgia. An attorney exercised at a gym in California. A political strategist went out on the stump in North Carolina. And a Cabinet secretary embarked on a three-state tour of manufacturing facilities.
Each had been in Washington days before, visiting the White House for a Sept. 26 ceremony introducing President Donald Trump’s Supreme Court nominee. The elegant affair, involving much of the country’s conservative elite, is now believed to have possibly contributed to a coronavirus outbreak sickening Trump and at least nine other members of his administration, in addition to top Republican officials and members of Congress and the military.
With no systematic effort to trace or advise the hundreds of guests at the Rose Garden ceremony and other events in the surrounding days, many made their way home and resumed their busy schedules, according to interviews with more than 40 people who attended events with the president between Sept. 25 and Oct. 1, when Trump announced he had tested positive.
Experts said the fallout, driven largely by individuals forced to make their own choices without clear instructions from a central authority, is emblematic of the nation’s response to the pandemic and helps explain why the virus remains uncontained nearly 10 months after it first arrived in the United States. The infection of Trump and those around him was, even more starkly, a window into an attitude of invulnerability and indifference that surrounds the president.
One of the people ensnared in the outbreak was Ronna McDaniel, the chairwoman of the Republican National Committee, who mingled with donors at a Sept. 25 event headlined by Trump at his hotel in Washington. She tested positive for the virus five days later but only made her diagnosis public on Oct. 2 after informing the president that morning. A person close to her said she attempted to reach the president sooner but was unable to talk to him.
For 36 hours after her diagnosis, the RNC made no attempt to inform donors who had attended the extended, indoor fundraiser with McDaniel. Only on Oct. 2, after the president had also tested positive, were attendees told they might have been exposed.
Guests of the president and his campaign returned to at least 20 states, often by plane. They visited college campuses and sat across the dinner table from elderly parents. They attended church and addressed crowds at indoor conventions, including on the topic of election security.
Upon learning they may have been exposed, some chose to quarantine or get tested. Others were waiting instead to see if they developed symptoms – despite months of warnings from scientists that it is possible to be contagious without feeling ill.
And in many cases, the attendees said they were not worried, expressing faith in the health precautions taken by their hosts despite the outbreak.
“Feeling tiptop,” said Frank Cannon, a conservative strategist, upon returning from a campaign swing through North Carolina in support of Republican Sen. Thom Tillis, who attended the celebration for Judge Amy Coney Barrett and later tested positive. Cannon also attended the Sept. 26 event but said he used a rapid test and received a negative result.
“I would go to such an event again,” said Yechezkel Moskowitz, 33, a venture capitalist from Long Island who attended a Sept. 30 fundraiser at Trump’s Bedminster, N.J., club. “I felt safe.”
Trump attended the Bedminster fundraiser even though a close aide, Hope Hicks, had tested positive for the coronavirus earlier in the day. A timeline compiled by the RNC indicates the president was inside with donors for about 65 minutes, hours before he announced his positive test. He did not wear a mask. A list provided to state authorities showed he was around more than 200 people
The reaction to the outbreak was notably different in the communities where the events occurred, and in some of the places to which guests returned, where businesses temporarily shuttered or quarantined staff after contact with associates of the president. People have gone into quarantine from Minnesota to Massachusetts Avenue, bracing for possible secondary infections.
Holy Angels, a nonprofit run by the Sisters of Mercy in Belmont, N.C., which provides jobs and other opportunities for people with disabilities, closed three of its businesses on Oct. 2 for a day of deep cleaning following a surprise visit from Ivanka Trump, the president’s daughter and adviser, who reported a negative test that day.
Sister Nancy Nance, vice president of community relations for Holy Angels, said the group took precautions not knowing immediately the status of Trump’s daughter or of others in her entourage. She said the businesses had just reopened after about six months in which they were closed to protect the medically fragile population served by Holy Angels.
“I don’t think the White House as a whole has handled the covid-19 pandemic appropriately,” Nance said. “They’ve downplayed it, and now it’s pushing people like me into a political arena that I don’t want to be in.”
Some guests said they regretted participating in the events, despite extensive security procedures that made them feel safe at the time. Guests in the Rose Garden described multiple checkpoints where attendees were required to wear masks, though many later took them off once seated.
“There was a false sense of security, being in the presence of people around the president who had been tested,” said one person who was pictured in the Rose Garden hugging Sen. Mike Lee, R-Utah, and shaking hands with Chris Christie, the former governor of New Jersey. Both have since tested positive. “I’ve thought about it, and talked to my wife, and that’s a good lesson learned,” said the attendee, who had received one negative test and was considering whether to take another, and who spoke on the condition of anonymity to discuss private health matters.
None of those interviewed by The Washington Post said they had been contacted by the federal government with questions about possible symptoms of covid-19 and contacts over the past 12 days. None had been advised by federal authorities about protocol to keep others safe during a period in which an infection could still develop, previous negative tests notwithstanding.
Rebekah Holler Ashworth, whose brother, Lance Cpl. Luke Holler, was killed in 2006 by a roadside bomb in Iraq, said she and her relatives – a group of seven – traveled from Texas for a Sept. 27 White House event for Gold Star families. She said that she had not been contacted by the White House but that no one in her family had become ill.
“No one has gotten sick,” Ashworth said. “I felt like everything was handled so well, and we were very comfortable. It was a phenomenal event.”
The White House says it is tracing contacts only for the 48-hour period preceding the president’s positive test, in line with the Centers for Disease Control and Prevention’s definition of a “close contact.” If someone falls into that time frame, said White House spokesman Judd Deere, the “Medical Unit makes appropriate notifications and recommendations.
“Any positive case is taken very seriously, which is why the White House Medical Unit leads a robust contact-tracing program with CDC personnel and guidance to stop ongoing transmission,” he said.
That approach means administration officials may never learn how the coronavirus was introduced into the president’s bubble, disease investigators said. Nor will the federal government be able to identify and help contain the possible secondary infections spawned from a series of bustling events, both indoor and outdoor, attended by people now reporting infections – from the glitzy event for donors at the Trump International Hotel on Sept. 25 to the fundraiser at Trump’s golf course in Bedminster on Oct. 1.
“If there are indications that events look like seats of activity and spread, even if they occurred more than 48 hours before the onset of symptoms or a positive test, then it certainly pays to interview those people,” said Jeffrey Koplan, a former director of the Centers for Disease Control and Prevention. “But the process may reveal information that this White House doesn’t want, magnifying the incredible crisis induced by this organism.”
For the Rose Garden event – as for the Trump hotel fundraiser and the event in the East Room for families of deceased U.S. troops – anyone expected to come into contact with the president submitted to a rapid test, which can provide results in 15 minutes but is less reliable than the more common tests that take three to five days. For the Rose Garden event, that included pastors who prayed with Trump and those who joined him afterward for an indoor reception. Several who remained outside recalled submitting to no more than a temperature check.
Beyond these precautions, designed to protect Trump from the public but hardly guaranteeing the safety of those around him, social distancing was not uniformly observed, according to public photos and interviews with attendees. Few guests consistently wore masks.
The high-ranking government officials, prominent media personalities, wealthy donors and well-connected lobbyists who attended the events preceding the president’s diagnosis have access to the best scientific information in the world, said Ross Goldberg, president of the Arizona Medical Association. They still flouted widely known best practices like mask-wearing and social distancing.
At least two of the people infected – Christie and Kellyanne Conway – attended debate prep, the Rose Garden ceremony and a VIP party inside the Diplomatic Reception Room. White House officials have not yet determined where they contracted the virus. Several aides who had been in close contact with Hicks said they only learned many hours later, and often through secondhand channels.
Rich Roberts, a physician and retired pharmaceutical executive who attended the Bedminster fundraiser, said in an interview that he had assumed that the rapid coronavirus test administered by the Secret Service would have been highly accurate and used cutting-edge technology. Roberts said he was not worried about catching the virus from other attendees, believing that even if they had contracted the virus, their negative test result would likely mean that they were not contagious.
If he knew what test the Secret Service administered, and that it had a significant false-negative rate, he would not have attended the event, Roberts said in an interview. He also said that calls to contract-trace the White House outbreak don’t make much sense to him, because of what he views as the near-impossibility of tracking the movements of so many people who entered the president’s orbit and then returned to their own lives.
“This is not like a linear handoff of a baton,” Roberts said, likening the quest to contain the White House cluster to a relay race. “This is lots of batons flying in many directions for everyone.”
Goldberg, the Arizona doctor, said the batons have been dropped.
“You couldn’t design a better example of how this thing spreads when people let their guard down, or deny the reality of the virus,” he said.
Because there was no immediate effort to interview guests at White House and campaign events about possible symptoms or to trace their contacts, responsibility fell to local health departments, which took different approaches. Otherwise, most attendees assessed their risk on their own.
One Washington lobbyist who attended the Rose Garden event said he sought out a rapid test last week because “I came back from that event and my wife was like, ‘I saw the photos, and there was not a lot of social distancing.’ “
Health officials in Mecklenburg County, N.C., said they were conducting a case investigation and contact tracing related to Tillis, “as we do with all positive results on county residents.” In Pennsylvania, health authorities encouraged attendees of the president’s Sept. 26 rally at the Harrisburg International Airport to download the state’s covid-19 app.
But a local case investigation was yet to begin for Greg Laurie, the pastor at a megachurch in Riverside, Calif., who tested positive after returning from the Rose Garden event and a prayer march the same day on the National Mall, said a spokesman for the county health department.
“At this point that church has not communicated with us,” said the spokesman, Jose Arballo.
A spokesman for Laurie said he “thought the labs/testing centers are the ones who report the cases.” In a video posted on Facebook, the pastor said, “I just wish that at a time like this, we could not politicize something like this and show compassion to people that are struggling with this.”
Jentezen Franklin, senior pastor of Free Chapel in Gainesville, Ga., posted a video on social media a week after he had attended the Rose Garden ceremony expressing excitement for church. “Get your family there,” he said. “We’re going to social distance. We’re going to wear masks.”
Beyond the individual decision to get tested, there was no central mechanism for tracking and preventing possible spread from the events in Washington.
At the fundraiser at Trump’s hotel, donors paid up to $100,000 a head to participate in a roundtable event, including taking a photo with the president. McDaniel, the RNC chairwoman, attended the roundtable and a dinner with donors after.
Guests were instructed to wear masks while awaiting the results of rapid tests, several who attended said. Each was then given a piece of paper reporting their results.
That sheet specifically alerted attendees that the tests are not fail-safe and sometimes produce false negatives, one donor said. Nevertheless, after testing negative, attendees were permitted to remove their masks. Neither McDaniel nor the president wore a mask, attendees said.
Attendees said efforts were taken to keep them more than six feet away from the president. Guests were photographed standing a distance from the president and were told that the images would be altered to make it appear as though the president was standing next to each donor. Updated CDC guidance suggests the virus can spread beyond six feet indoors.
No such precautions were taken for McDaniel, who mingled freely with others. Among those in attendance was Labor Secretary Eugene Scalia.
The next day, Scalia and the president attended the Rose Garden ceremony, while McDaniel returned to her home in Michigan, said a person close to McDaniel, who spoke on the condition of anonymity to share private information.
By Monday, McDaniel had begun experiencing a sore throat and fatigue, the person said. The person said McDaniel believed she may have contracted the virus upon her return home from a family member who had tested positive earlier in the week but whom she had not seen for 17 days before her return. During her absence she had also been traveling extensively and meeting with donors and supporters, at times without a mask.
The person said McDaniel called the White House on Sept. 28 to inform the president that she was not feeling well and had decided to skip his debate the following day. It was not clear whether the White House took any steps in response to the news that the party chairwoman was experiencing symptoms.
That same day, McDaniel sought a test for the coronavirus, the person said. The results did not come back until Sept. 30 – after the president had spent significant time interacting with aides and family and attending the debate in Cleveland. The test was positive.
At that point, McDaniel attempted to reach the president to inform him of her results but was unable to get through. Again on Thursday, she tried and failed to inform the president. She eventually reached Sean Conley, the White House doctor. Other White House aides have said they were not aware of her diagnosis.
Mike Reed, an RNC spokesman, said McDaniel tested negative the day of the fundraiser, as well as the day before.
“She went home early the next morning and began to feel symptoms the following week after being exposed to a member of her immediate family who tested covid-19 positive,” Reed said. “This was the chair’s first contact with this family member since the individual tested positive, so there was no reason to believe she had the virus the week prior.”
He said more than 40 staff members who interacted with McDaniel before she returned to Michigan are all feeling well and have tested negative for that coronavirus and that RNC officials have been in contact with donors who attended the fundraiser and that none have reported symptoms or positive tests.
Following the weekend events, Scalia resumed his busy schedule as a Cabinet secretary. That Monday, he began a tour of manufacturing facilities, wending his way through Ohio, Pennsylvania and New York for roundtable events with workers. That Wednesday, he joined Karen Pence, the wife of Vice President Mike Pence, at a naval air station in Jacksonville, Fla., to announce a new program to assist military spouses. Photographs of the events posted on Twitter show Scalia and others wearing masks.
A spokesman for the Labor Department said Scalia is “frequently tested,” adding that all of his tests have come back negative. He did not provide a date of Scalia’s most recent test. One of his brothers, the Rev. Paul Scalia of the St. James Catholic Church in suburban Virginia, apologized to his parish for attending the ceremony without a mask.
Health officials in Minnesota, where the president attended a fundraiser Tuesday, the day before his diagnosis, said they had not been in contact with the White House, the president’s campaign or the RNC and did not have a list of those who had attended events in the state.
Meanwhile, 13 staffers at Murray’s, a historic downtown Minneapolis steakhouse, had been quarantined after catering a $7 million fundraiser that Trump attended in Shorewood, Minn., on the evening of Sept. 30. In a statement, Chuck Sanger, a restaurant spokesman, said the staff did not come into contact with Trump. But upon learning of the president’s diagnosis, the restaurant had immediately enacted a 14-day quarantine and asked the staffers to get tested.
By Syndication Washington Post, Bloomberg · Suzi Ring · WORLD, HEALTH, EUROPE, HEALTH-NEWS A covid-19 vaccine is looking “unlikely” by year-end, according to the head of the European medicines regulator, even as the agency conducts accelerated reviews of two front-runners for a successful shot.
“Technically, of course it’s possible. Practically it’s very difficult — it’s very unlikely,” said Guido Rasi, executive director of the European Medicines Agency, in an interview Thursday. Even if drugmakers “submit the data in a few weeks, we are already approaching middle of October, so if we wait a few weeks and we take a minimum time of evaluation, more or less we are at the end of the year.”
Pressure is mounting globally for a vaccine as infection rates soar and countries revisit lockdown measures. In recent weeks, the EMA started two so-called rolling reviews — real-time evaluations of data to speed up potential approvals — of jabs from AstraZeneca and the University of Oxford, and from Pfizer and BioNTech. In the U.S., getting a shot through by the November election, President Donald Trump’s desired deadline, also looks increasingly unlikely.
The first vaccines will probably be given conditional marketing authorizations, according to Rasi. These are temporary, one-year approvals granted when the benefit of having a product immediately available outweighs the risk of less substantial data. Regulators would need to know the duration of immunization for a vaccine before granting a full marketing clearance, he said.
It’s still possible that countries in the European Union could use national emergency powers to distribute a vaccine before the EMA approves one. The U.K. set out plans in August to amend legislation and clarify its powers so that an unlicensed covid-19 shot could be temporarily authorized in Britain. But this could create confusion around safety, and countries would do better focusing on their vaccine distribution plans than trying to have a shot “a few days before,” according to Rasi.
“I really discourage” the thought of EU countries going it alone, he said. If a country tries to go ahead of the EMA, it might be “perceived as though this rush is not giving us all the reassurance about the safety and efficacy, so might just fuel vaccine hesitancy.”
Asked about the U.S. regulator’s decision to continue to pause Astra’s final-stage trial in America, Rasi said he thought the Food and Drug Administration was very close to releasing its opinion and didn’t see the situation as a major issue. Astra told analysts this week that it expects an update in the next one to two weeks on the trial, which was halted after a U.K. participant fell seriously ill. Tests have already resumed in the U.K., Brazil and South Africa.
Rasi will step down as head of the EMA on Nov. 15, with Emer Cooke, a former colleague at the agency, set to replace him. She has been working as head of medicines regulation at the World Health Organization.
Europe battles to contain virus as cases spike across the region
Health & BeautyOct 08. 2020Pedestrians walk past a closed restaurant at night in Madrid, Spain, on Oct. 7, 2020. MUST CREDIT: Bloomberg photo by Paul Hanna.
By Syndication Washington Post, Bloomberg · Rudy Ruitenberg, Geraldine Amiel, Lenka Ponikelska, Naomi Kresge · BUSINESS, WORLD, US-GLOBAL-MARKETS, EUROPE
European countries stretching from Spain to Ukraine posted record increases in coronavirus cases, underscoring growing alarm in the region as it struggles to control the pandemic.
Local authorities are being pushed to take the lead in limiting late-night activity in cities and towns, as national politicians fear that more wide-ranging measures could result in another collapse in economic activity. Several cities, including Paris and Berlin, have imposed more severe restrictions to try to rein in the social activity blamed for helping spread the disease.
In France, President Emmanuel Macron’s government ordered bars in Paris to close for a two-week period and said more curbs will be announced later on Thursday. The Czech Republic is also considering additional steps.
“There must be more restrictions such as the ones put in place” in the region of Marseille, where bars and restaurants were shut, Macron said in a TF1 interview.
Daily infections in France increased by 18,746, health authorities said on Wednesday, bringing the seven-day rolling average to the highest level yet. Spain reported a record 5,075 new cases, while infections in Germany in the past 24 hours exceeded 4,000 for the first time since early April.
France’s health minister will announce measures on Thursday that will focus on places where the virus is circulating faster among elderly people and where hospitals are the fullest, Macron said. The number of covid-19 patients in intensive care in Paris hospitals has tripled since the start of September, similar to the situation in the Marseille region.
Like Paris, Berlin is fighting against a surge in infections and will close bars at 11 p.m., starting on Saturday.
The German capital has the worst outbreak among the country’s 16 states, with 40.5 cases per 100,000 people over the last seven days, according to the public health authority. The city’s residents would be restricted from domestic travel if the figure rises above 50. Some districts already exceed the threshold and one local newspaper, citing its own calculations, reported Thursday that the city as a whole had edged above it.
Coronavirus infections across the whole of Germany climbed by 4,010 in the 24 hours through Thursday morning, the highest since April 10, according to data from Johns Hopkins University. That brought the total to 311,137.
The numbers are “very worrying,” Health Minister Jens Spahn said at a briefing. While ruling out the idea of a second national lockdown, Spahn called for targeted local restrictions and appealed to individuals to avoid situations where the virus is likely to spread, such as indoor gatherings and poorly ventilated areas.
The pandemic is “a character test for us as a society,” Spahn said. “I want us to pass this test, and we can do it, but we can only do it together.”
Across the border from Europe’s largest economy, the Czech Republic on Thursday posted a record 5,335 new cases for the previous day. The country’s 14-day cumulative number of cases per capita is now the highest in the EU, surpassing Spain.
The government will announce “more significant” measures to stem the outbreak at the end of the week, Health Minister Roman Prymula said Wednesday, reaffirming a pledge not to impose another full-scale nationwide lockdown.
Austria also recorded a record number of daily infections on Thursday, with Vienna accounting for more than half of the 1,209 new cases. Ukraine recorded an additional 5,397 infections, which is also the highest one-day total.
In Poland, covid-related deaths jumped by a record 76 to 2,867 in the past 24 hours. The government is expected to announce measures to stem infections in Warsaw at a press conference later on Thursday.
The virus’s resurgence in Italy — where numbers have been more contained than in some neighboring countries — twice prevented parliamentary votes earlier this week on new measures to combat the pandemic, as a number of lawmakers were in quarantine.
A cabinet meeting chaired by Prime Minister Giuseppe Conte extended emergency powers to counter the pandemic to Jan. 31. The government again made wearing face masks outdoors compulsory nationwide.

 เทรนด์มาแรง “เครื่องดื่มเพื่อสุขภาพ” อุดมด้วยโปรตีนจากพืช รับกระแส “วีแกน” ไม่บริโภคเนื้อสัตว์ ลดเสี่ยงโรคห่างไกลมะเร็ง
เทรนด์มาแรง “เครื่องดื่มเพื่อสุขภาพ” อุดมด้วยโปรตีนจากพืช รับกระแส “วีแกน” ไม่บริโภคเนื้อสัตว์ ลดเสี่ยงโรคห่างไกลมะเร็ง


 เช็กตัวเองกันสักนิดว่าบริโภคโซเดียมเกินลิมิตหรือเปล่า?
เช็กตัวเองกันสักนิดว่าบริโภคโซเดียมเกินลิมิตหรือเปล่า?
 Physician Peter Chang tracks coronavirus indicators, including hot spots in Tampa, where he works at Tampa General Hospital. MUST CREDIT: Washington Post photo by Michael S. Williamson.
Physician Peter Chang tracks coronavirus indicators, including hot spots in Tampa, where he works at Tampa General Hospital. MUST CREDIT: Washington Post photo by Michael S. Williamson. 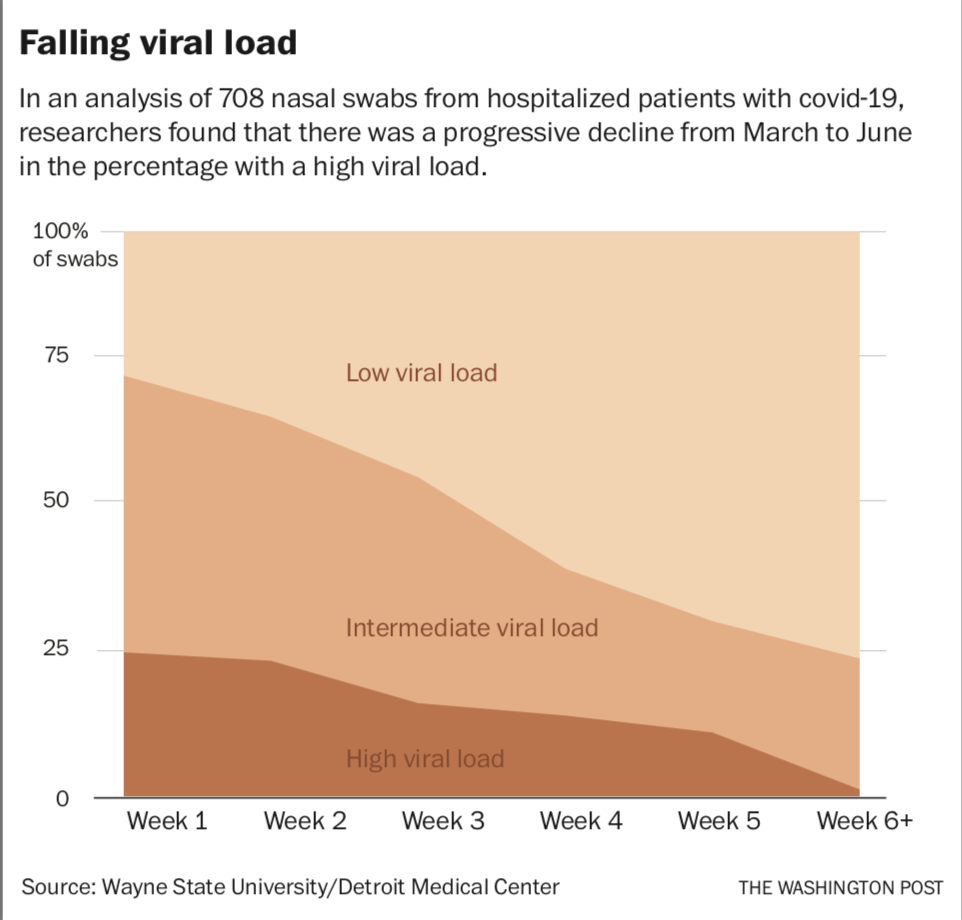






















 8 ตุลาคม 2563 – 20:20 น.
8 ตุลาคม 2563 – 20:20 น.





 People listen as President Trump announces Judge Amy Coney Barrett as his nominee to the Supreme Court in the Rose Garden on Sept. 26. MUST CREDIT: Washington Post photo by Jabin Botsford
People listen as President Trump announces Judge Amy Coney Barrett as his nominee to the Supreme Court in the Rose Garden on Sept. 26. MUST CREDIT: Washington Post photo by Jabin Botsford 
 Pedestrians walk past a closed restaurant at night in Madrid, Spain, on Oct. 7, 2020. MUST CREDIT: Bloomberg photo by Paul Hanna.
Pedestrians walk past a closed restaurant at night in Madrid, Spain, on Oct. 7, 2020. MUST CREDIT: Bloomberg photo by Paul Hanna. 