WASHINGTON – Temperature-scanning devices that check for fevers in schools, workplaces and public venues across the United States distort the results in a way that could overlook the telltale sign of a coronavirus infection, according to new research that casts doubt on the systems’ effectiveness in helping people resume normal life.
The thermal cameras and “temperature tablet” kiosks have been heralded as a critical first line of defense against new pandemic outbreaks. But in a new study of the scanners by the surveillance research organization IPVM, researchers warn that the tools are dangerously ineffective, raising the risk that infected people could be waved through medical screening checkpoints and go on to spread the virus unchecked.
On Thursday night, shortly after The Washington Post discussed the research findings with the Food and Drug Administration, the agency issued a public alert warning that improper use of the devices could lead to inaccurate measurements and “present potentially serious public health risks.”
The agency also announced that it was sending official “warning letters” to one of the discussed companies, as well as three others, for selling “unapproved, uncleared, and unauthorized thermal imaging systems.”
In the letter to the company, Certify Global, FDA officials said use of the devices carried the risk of incorrect detection, particularly if used to scan multiple people simultaneously, and that a person with an undetected fever may “be less likely to adhere to infection prevention and control guidelines.”
The researchers found that seven widely used scanners attempt to compensate for the imprecisions of lower-cost sensors and the unpredictable factors of real-world tests by “normalizing” the readings of people’s temperatures.
But that “compensating algorithm,” they argue, severely undermines the devices’ medical usefulness. A feverish person with a core temperature of 100.4 degrees, their research found, could be assessed by the test devices as having a temperature of 98 degrees, well within the healthy range.
“The utility of these devices as fever screeners is now highly questionable, and arguably a risk to public health, because they actively report fevers as normal,” said Conor Healy, the lead researcher of the study set for publication in the Journal of Biomedical Optics.
Representatives of the tested companies Certify, Dahua, Meridian and ZKTeco disputed the findings, saying their systems don’t manipulate temperature readings but in some cases use software techniques to “self-calibrate” to their environment.
“The deviation setting is not intended to ‘distort’ results. It’s designed to allow customers to receive alerts only when actual threats exist,” said Larry Reed, the chief executive of ZKTeco, which makes a “SpeedFace” thermal-imaging system that sells for about $3,800. “On a hot summer day in Arizona, [non-feverish] employees might trigger the device alarm all day if it’s set at 101 degrees and the employees are scanned upon immediately entering the building.”
Peter Plassmann, a thermography expert whose U.K.-based company Thermetrix designs thermal-imaging systems for medical use, said the research highlights how companies have sought to bolster their business by oversimplifying how well the devices are supposed to work.
“That’s generally the problem with infrared imaging: It’s so deceptively easy,” he said. “You point the camera at somebody, you get a nice colorful image and you get a temperature reading. Great. But in reality, it’s all rubbish. There are so many factors you need to consider.”
Companies have promoted the thermal-imaging systems for their ability to measure temperatures more quickly and at a safer distance than traditional and infrared thermometers that measure temperature from a person’s forehead, ear or mouth.
The scanners use infrared sensors to analyze the heat radiating from a person’s skin – a close but imperfect reflection of their core body temperature – and some systems are advertised as being able to assess multiple people in a passing crowd.
The FDA typically requires thermal scanners and other medical-use devices be tested for safety and effectiveness under a process known as 510(k) clearance. But in April, the agency said it would no longer require premarket reviews or object to unvetted devices that did not “create an undue risk.”
A surge of new thermal scanners followed, said the researchers, who counted more than 200 companies now making or advertising such devices. Many of the companies first jumped into the market last year without any previous experience in thermal-imaging or medical devices.
The FDA has said the change was a necessary move to address fears of device shortages. But the researchers said they worry that such untested systems are now widely distributed across the country and could fuel a “false sense of security” that could imperil public health.
Thermal scanners face a huge flaw in their ability to detect coronavirus infections: Roughly 40% of infected people won’t have a fever at all, the Centers for Disease Control and Prevention estimated last year. And a person’s temperature can shift wildly based on many factors, including if they’re overweight, stressed, menopausal or wearing heavy clothing, or if they recently exercised, stepped out of a hot car, or drank alcohol or caffeine.
But because there is no immediate alternative for detection, many officials have seen the fever scans as perhaps their only way of identifying someone who could spark a new outbreak. Some companies and local governments have spent tens of thousands of dollars per camera to bolster their defenses.
The FDA has worked to adjust Americans’ expectations about how useful the systems can be. The agency says in official guidelines that thermal scanners are “not effective at determining if someone definitively has covid-19”; that they “have not been shown to be accurate when used to take the temperature of multiple people at the same time”; that their accuracy depends heavily on “careful set-up and operation”; and that “their effectiveness as part of efforts to reduce the spread of disease has been mixed.”
Bill Maisel, the chief medical officer and director of the Office of Device Evaluation at the FDA’s Center for Devices and Radiological Health, said the research identified several systems that “didn’t have the level of accuracy that we would expect.” Even after the premarket review change last year, he said, the FDA still required all devices to meet certain performance expectations. The agency, he added, regularly monitors for problematic systems and works with the companies to address errors when their products are found to underperform.
The devices, he said, should play only a limited role when assessing risks during the pandemic, and they are no replacement for social distancing, mask-wearing or more traditional medical screening.
Thermal-imaging devices are “imperfect, and they are particularly imperfect when screening for covid,” he said. “The inaccuracy of devices is one of the aspects that contributes to the imperfection.”
The IPVM researchers did not test traditional thermometers, and their findings confirmed that some FDA-cleared devices returned near-perfect accuracy. But all of the thermal scanners they tested appeared to deliberately “normalize” high temperature readings into a healthier, non-fever-like range: Colder readings were pulled higher, while hotter readings were pulled down.
The tested systems relied on lower-cost hardware with dramatically lower precision: Several scanners used a sensor with a resolution of about 1,000 pixels – far more limited than the 76,000-pixel sensor found in one of the FDA-vetted machines they used as a control device.
To get an accurate temperature reading, international guidelines for medical electrical equipment say the systems should only be used in controlled environments with regularly calibrated devices on people who are consistently “prepared”: People walking in from an indoor waiting room, for example, would offer very different results than others who had lined up waiting in the sun.
But the companies, Healy said, appeared to navigate that challenge by making the systems appear to work consistently across a wide range of ever-changing conditions.
The systems, Healy said, were designed “to maintain an appearance of normal function despite poor device capabilities or screening conditions, enabling manufacturers to cover up performance issues while selling to a much wider set of use-cases.”
IPVM is a surveillance research group that examines camera hardware, imaging devices and other technical tools for its members, largely in the security industry. Its researchers examined the systems in a temperature-controlled warehouse laboratory in Pennsylvania.
The tested companies are not household names, but they form the technical backbone of the screening systems used in schools, retail stores and workplaces nationwide. The devices range in price, from $600 to $13,000, and are promoted as being able to conduct person-by-person entry scans or assess visitors en masse.
Certify, a Maryland-based seller of devices found in casinos and hotels, advertises on its website that it offers “the #1 Fever Detection & Thermal Scanning Solution in the Marketplace” and can “replace manual scanning.”
Certify spokeswoman Jasmine Neisser said the system does not alter high temperatures but does set a minimum temperature level that will return a 96 degree reading if the scan fails. The system, she said, “uses world-class manufactured sensors for thermal applications, which are rigorously tested for accuracy.”
Certify Vice President Tim Goodwin had said in a LinkedIn post that devices like the SnapXT Pro, its $2,000 thermal scanner with an eight-inch touch screen, could be found in “more than 75 percent of NFL stadiums.” An NFL spokesperson disputed that claim, saying the devices are used in roughly a dozen of the league’s 30 stadiums nationwide. (Neisser said that the comment related to the number of open stadiums when the post was written last year and that at the time Certify devices had been deployed in five of the eight stadiums then open to visitors.)
Plassmann said the medical-equipment industry standards for deploying such systems, which cover everything from the lighting and humidity of screening rooms to how much time people should acclimate before their test, are often ignored in the real world, where unpredictable conditions and public circumstances can vary wildly and skew the results.
He said he has seen an influx of companies that offer glossy marketing materials but little commitment to the best practices for public-health use, and he said he is concerned that their widespread deployment could undermine efforts to guard against new outbreaks.
“It needs to be done properly,” he said, “or it can do more harm than good.”
Covid-19 cases are slowly slowing down since the vaccine was introduced near the end of 2020. However, some people still don’t have confidence in the vaccine due to its possible side effects.
A survey conducted by the US Pew Research Centre on 12,648 respondents aged between 18-29 years showed four out of 10 people are afraid to get the Covid-19 jab.
The queen of country music Dolly Parton, 75, is one of the many celebrities calling on people to take the Covid-19 jab as she has.
Parton posted a video clip on Instagram and Twitter taking a shot and singing a ditty to the tune of her hit “Jolene”, inviting people to take the vaccine. She has more than 4 million followers on Instagram and 5.2 million on Twitter.
“I’m old enough to get it and I’m smart enough to get it,” Parton said. “I just want to say to all of you cowards out there – don’t be such a chicken squat. Get out there and get your shot.”
US President Joe Biden is also urging US citizens to not worry about the vaccine.
Former California governor and Hollywood star Arnold Schwarzenegger was also filmed getting a jab at a drive-thru vaccination clinic. He too called on people to take the Covid-19 jab like him if they want to live.
The US has launched the Covid-19 vaccination programme for more than 50 million people. Biden’s aim is to have up to 100 million people vaccinated within the first 100 days of his presidency. The US is expected to reach this target by April 30.
In Thailand, the Covid-19 vaccine has arrived.
The Economist Intelligence Unit expects everybody in Thailand to be vaccinated against Covid-19 by the end of 2022.
Have you ever thought that Thais are getting taller as the years go by? Well now it’s official: The Public Health Ministry has raised its standard height for Thai children, men and women.
The development criteria for children aged 6-19 have been adjusted upwards from the standards used since 1995, said Deputy Public Health Minister Satit Pitutacha.
The decision was made because the latest generation of Thai children was outgrowing the previous standard for both height and weight. Under the 1995 standard, the average height of Thais at age 19 is 165 centimetres for men and 159cm for women. According to the new standard the average height five years from now (2026) will be 175cm for men and 162cm for women. In 15 years (2036), Thai men will average 180cm and women 170cm.
The new growth criteria will be supported by information on correct nutrition and exercise to strengthen joints and increase height, said the ministry.
By The Washington Post · Laurie McGinley, Christopher Rowland
WASHINGTON – President Joe Biden announced Tuesday that pharmaceutical giant Merck will help make Johnson & Johnson’s single-shot coronavirus vaccine – an unusual pact between fierce rivals that is among several steps intended to boost supply as Biden pushes toward having enough shots for every adult by the end of May.
Biden hailed the development as an example of industry coming together for the common good, in keeping with his frequent calls for a stronger emergency footing to combat the pandemic.
“Two of the largest pharmaceutical companies in the world who are usually competitors are working together on the vaccine,” he said in remarks delivered at the White House. “This is the type of collaboration between companies we saw in World War II.”
Biden’s vow to produce enough vaccine for all U.S. adults by the end of May is two months faster than his previous goal of the end of July. But the Merck deal on its own is not expected to ramp up fast enough to impact vaccine supplies significantly in the next three months.
Biden officials have successfully pushed Johnson & Johnson in other ways: The company and its contract manufacturers are moving to round-the-clock production, posting full-time technicians in plants to immediately repair any machinery breakdowns, and accepting daily logistical help from the Department of Defense, the administration said.
“Among the things I learned when I came into office was that Johnson & Johnson was behind in manufacturing and production,” Biden said. “We had the potential to have a highly effective vaccine to accompany the two existing vaccines. It simply wasn’t coming fast enough.”
Rather than a vastly accelerated timeline, Biden’s revised May target reflects his administration’s new confidence in the schedules set forth by all of the vaccine manufacturers. An administration official said Johnson & Johnson’s latest goal is to produce 94 million doses of its single-shot vaccine by the end of May – that is about 7 million doses ahead of the schedule in its contract, which calls for delivery of 87 million doses by the end of May and the full 100 million by the end of June.
With Pfizer and Moderna already pledging to deliver 200 million doses each of their two-shot vaccines by late May, the total supply would be more than enough for the estimated 260 adults living in the United States currently eligible for a coronavirus vaccine.
The Merck deal is geared toward the second half of the year, an administration officials said. That’s when the threat of variants could loom larger, requiring the manufacture of booster shots, and also when greater political attention will turn to supplying the developing world with vaccine.
The administration will pay $268.8 million to Merck to upgrade multiple plants to the necessary safety standards to produce Johnson & Johnson vaccine, from fermentation in vats to final finish and filling in vials. The Biden administration and the companies did not disclose the number of doses Merck would produce for Johnson & Johnson.
Biden’s team began scouring the country for additional manufacturing capacity soon after taking office, according to administration officials who spoke on the condition of anonymity before Biden’s announcement.They soon sought a deal with Merck, one of the world’s largest vaccine makers, which had failed to develop its own coronavirus vaccine.
Under the arrangement, Merck will dedicate two facilities in the United States to Johnson & Johnson’s shots. One will provide “fill-finish” services, the last stage of the production process during which the vaccine substance is placed in vials and packaged for distribution. The other will make the vaccine, and has the potential to vastly increase supply, perhaps even doubling what Johnson & Johnson could make on its own, the officials said.
Merck’s participation sets up a race to see how quickly it can make an impact on Johnson & Johnson’s rollout. It could easily take two months to get the “fill-finish” plant ready and a few more months to equip the other facility to make the vaccine, according to a person familiar with the process who spoke on the condition of anonymity because he was not authorized to discuss the issue.
Merck said Tuesday it would use the federal emergency money for vaccine-related upgrades as well as enhancements for production of unnamed drug treatments. After abandoning two vaccine candidates because they didn’t work, Merck still has two potential covid 19 treatments in its clinical trial pipeline.
“This funding from [the U.S. government] will allow us to accelerate our efforts to scale up our manufacturing capacity to enable timely delivery of much needed medicines and vaccines for the pandemic,” said Mike Nally, executive vice president, Human Health at Merck.
Johnson & Johnson said Merck’s involvement would permit it to go beyond the 100 million doses it has pledged to provide the United States under a $1 billion contract, but it did not provide any specifics.
“We think it’s going to add considerably to our capabilities, both near and long term,” Johnson & Johnson CEO Alex Gorsky told CNBC on Tuesday.
Biden is wielding the powers of the Defense Production Act, a Korean War-era law, to give Merck priority in securing equipment it will need to upgrade its facilities for vaccine production, including the purchase ofmachinery, bags, tubing and filtration systems.
In teaming up with Merck, Johnson & Johnson has a partner with a century-long tradition of making vaccines. In the United States, Merck is the sole supplier of the combination childhood vaccine that protects against measles, mumps and rubella. It developed Gardasil, which protects against the human papillomavirus. And it won Food and Drug Administration approval for an Ebola vaccine in 2019.
But the company, which makes vaccines in North Carolina, Pennsylvania and elsewhere, encountered setbacks in its quest to develop a coronavirus vaccine. Merck announced Jan. 25 that it was halting work on two experimental shots for the virus. The vaccine did not stimulate enough antibodies in Phase 1 human clinical trials to justify continuing, the company said.
Johnson & Johnson has been searching the world for manufacturing sites where it could produce doses of its vaccine on a global scale. It has publicly disclosed more than half a dozen manufacturing sites on four continents that it said were winnowed from more than 100 possibilities.
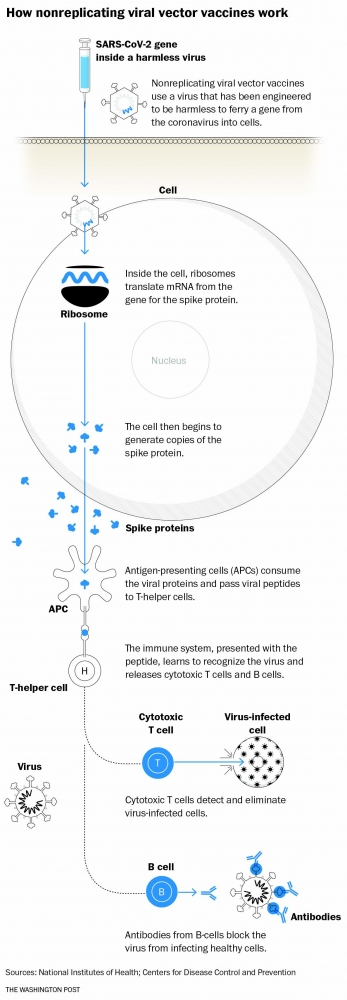
Its vaccine uses an adenovirus vaccine as a vector – a harmless cold virus that does not replicate in the body – to deliver DNA instructions into a healthy human cell. The cell uses the genetic instructions to create a replica of a coronavirus spike protein that triggers an immune response that can recognize – and respond to – the real thing. The U.S. government paid the company $2 billion for development and clinical trials and preorders at a price of $10 per dose just days after it received emergency authorization from federal regulators.
After the FDA on Saturday authorized the Johnson & Johnson vaccinefor use in those 18 and older, the company said it would immediately ship nearly 4 million doses in the United States, and a total of 20 million by the end of March, which is 17 million less than expected under its government contract.
Its current schedule calls for a recovery from those delays, with the company saying it is on track to deliver 100 million doses by the end of June. A top company executive told Congress last week that it has a goal of manufacturing 1 billion doses worldwide by year’s end.
Most of Johnson & Johnson’s partnersdisclosed to date are contract manufacturing companies, but now it is moving to team with larger drug companies that have seen their own vaccine projects delayed or fizzled.
Sanofi – which had to reboot its clinical trials of a vaccine candidate after early stumbles – announced last week that it would help Johnson & Johnson with final production steps and bottling in vials in Europe. Projected capacity from a Sanofi plant in France is 12 million doses per month.
BioNTech, Pfizer’s German partner on its mRNA vaccine, also announced deals in January for rivals Sanofi and Novartis to fill and finish vaccine vials in Europe.
The manufacturing process is time-consuming: Johnson and Johnson ferments large batches of its vaccine in vats at a contract manufacturing facility in Baltimore operated by Emergent, as well as locations in the Netherlands and India. That brewing step takes two months.
Emergent received commitments of $628 million from the Trump administration in June to expand capacity at its Baltimore plant for coronavirus vaccine production. It then received contracts worth $615 from Johnson & Johnson in July.
But eight months later, the undisclosed number of J&J vaccine doses produced at Emergent are not available for public distribution. Emergent still has not been authorized to produce Johnson & Johnson’s vaccine under the FDA emergency use authorization, the New York Times first reported Tuesday. An administration official said Emergent’s Baltimore production line is expected to be approved in the next few weeks.
After fermenting in vats, the vaccine needs to be put into its final formulation and packaged into vials for shipping, which takes another five to six weeks, including testing for purity. In the United States and Europe, that final “fill-finish” process for vaccines has created bottlenecks across the industry, as manufacturers have flooded the supply chain with demand to finish hundreds of millions of doses.
Johnson & Johnson has agreements for fill-finish work to be done by two companies in the United States: Grand River Aseptic, with plants in Michigan, and Catalent, at a plant in Indiana. Catalent also isperforming fill-finish operations for Moderna, which is obligated to deliver 300 million doses of its mRNA vaccine to the government by the end of July.
In Italy, Catalent also is helping Johnson & Johnson and AstraZeneca manufacture their vaccines.
Catalent said Tuesday that it had sufficient, dedicated capacity at its Bloomington, Ind., plant to handle the vaccine volume for both companies.
“Catalent is on track to deliver on our commitments for Johnson & Johnson coronavirus vaccine deliveries as soon as we are approved to begin shipments by the FDA, which we anticipate in the coming weeks. Catalent is also on schedule to meet our commitment to Moderna to produce 100 million doses by the end of March 2021,” company spokesman Chris Halling said in an email.
The Food and Drug Administration authorized Johnson & Johnson’s coronavirus vaccine for emergency use for people 18 and older on Feb. 28. (Reuters)
By The Washington Post · Lena H. Sun
WASHINGTON – A federal advisory panel voted unanimously Sunday to recommend the nation’s third coronavirus vaccine for people 18 and older, opening the way for the one-shot, easier-to-use Johnson & Johnson vaccine to be administered starting this week.
Meeting in emergency session, advisers to the Centers for Disease Control and Prevention strongly endorsed the vaccine’s effectiveness in completely protecting against hospitalization and death. The Johnson & Johnson vaccine is the first one authorized in the United States that does not need to be kept frozen or followed by a second shot.
The clearance of a third vaccine comes at a critical time in the pandemic: After weeks of steadily declining new cases in the United States, the downward trend has stalled – “a very concerning shift in the trajectory,” CDC Director Rochelle Walensky said Friday. Experts worry that state and local officials are relaxing restrictions too quickly, and people are letting down their guard even as more contagious and possibly, deadly virus variants are on the rise. It was almost one year ago that authorities announced what was believed to be the first coronavirus death in the United States. Since then, more than 500,000 deaths of covid-19, the disease caused by the coronavirus, have occurred in the United States.
“Covid cases and deaths are decreasing,” said Beth Bell, a global health expert at the University of Washington who leads the panel’s coronavirus vaccine working group. “But the pandemic is very far from over and many challenges are before us. The need for more safe and effective vaccines remains urgent and vital to ending the pandemic.”
The action by the Advisory Committee on Immunization Practices follows the Food and Drug Administration’s action Saturday in authorizing the vaccine for emergency use for people 18 and older. Walensky is expected to approve the panel’s action shortly after the vote, making it an official CDC recommendation to health providers.
The doses are expected to start shipping as early as Monday to sites already receiving doses of the authorized vaccines made by Pfizer-BioNTech and Moderna. Those locations include state health departments, pharmacies, federally qualified health centers and community vaccination centers.
Johnson & Johnson’s initial supply will be limited – nearly 4 million doses are expected to be shipped this week, and an estimated 20 million doses by the end of March, officials have said. But state officials already know what to expect because the number of anticipated doses for all three vaccines was included in information they received last week.
The Johnson & Johnson vaccine was 85% effective at protecting against severe cases of illness in late-stage trials, and there were no deaths or hospitalizations a month after participants received the vaccine. The vaccine was slightly less effective at preventing moderate illness (72% effective in the United States) where more-transmissible variants have only recently begun to be detected. Some experts are worried that the public will fixate on that data point and pass up getting the Johnson & Johnson shot in favor of other vaccines that underwent trials at an earlier stage of the pandemic when such variants were not a factor.
Panel members said that doing so would leave people unprotected and delay an end to the pandemic.
Officials stressed that vaccines were tested at different times, against different circulating variants and in settings with different levels of transmission.
“While there are differences in efficacy of the three vaccines for moderate illness, the more severe the outcome, the more similar the efficacy,” said Saad Omer, director of the Yale Institute for Global Health who is not a member of the panel. “In other words, we now have three highly effective vaccines available in the U.S. – particularly against severe outcomes such as hospitalization and death. This one-dose vaccine, that can be stored at refrigerator temperatures, is likely to enhance the ability of health departments and health systems to conduct mass vaccination. The rate limiting step remains availability of doses.”
Members and immunization advocates expressed concern that information about the vaccine’s efficacy will be confusing for the public and make it even more difficult to get shot to hard-to-reach communities.
“We need some real plain language and clear public education on the difference between clinical trial efficacy and real world effectiveness,” Karen Ernst, who heads Voices for Vaccines, a parent advocacy group, said during the public comment period.
The second Covid-19 vaccination may cause fewer side effects compared to the first jab, Chulalongkorn University’s Centre of Excellence in Vaccine Research and Development director Kiat Rakrungtham said on Sunday.
He said only one of 1 million people have side effects due to the Covid-19 jab.
“The vaccine’s side effects are fever, aching muscle and pain in the spot where the jab was given,” he said.
He added that the vaccine will give maximum protection to people after receiving the second dose.
“Until then people still have to undergo measures to contain the spread of Covid-19, such as wearing face mask, washing hands and maintaining social distance,” he added.
Public Health Minister Anutin Charnvirakul became the first Thai person to be vaccinated against Covid-19 at Bamrasnaradura Infectious Diseases Institute in Nonthaburi province at 7.45am on Sunday.
Anutin was followed by Public Health Deputy Minister Sathit Pitutecha, Culture Minister Itthiphol Kunplome, Public Health permanent secretary Kiattiphum Wongrajit, Department of Disease Control director-general Opas Karnkawinpong and Education Deputy Minister Kanokwan Wilawan.
Chulalongkorn University virology specialist Dr Yong Poovorawan and medical personnel administered the Sinovac Covid-19 vaccine to the Cabinet members and senior government officials on Sunday morning.
Prime Minister Prayut Chan-o-cha was present as well to oversee the vaccination drive.
By The Washington Post · Laurie McGinley, Carolyn Y. Johnson
WASHINGTON – The Food and Drug Administration late Saturday granted emergency use authorization to Johnson & Johnson’s single-dose coronavirus vaccine, providing the United States with a long-anticipated tool that adds firepower and flexibility to the nation’s accelerating inoculation effort – but also presents new challenges.
Health authorities now have three effective vaccines, a singular scientific achievement that few would have predicted a year ago, when a pandemic emerged that has killed 2.5 million people worldwide, including more than 500,000 in the United States. It comes at a particularly fraught time, as Americans are whipsawed by encouraging developments, including sharp declines in nursing home deaths, and concerning news such as the emergence of potentially menacing variants.
With demand for vaccines outracing supply and officials scrambling to get much of the population vaccinated before variants spoil an improving picture, a third vaccine is “really good news,” said Eric Toner, senior scholar with the Johns Hopkins Center for Health Security. The vaccine will not have a big effect initially on supply shortages. Only a few million doses will be shipped to states in the days immediately after authorization, though production will ramp up in coming weeks, with 20 million doses to be delivered by the end of March and 100 million total in the first half of the year, according to the company.
The new vaccine has clear practical and logistical advantages over the first two vaccines – it does not have to be kept frozen, and there is no need for a second round of appointments. That makes it a boon for rural areas and other hard-to-reach communities, and for distribution to community health centers and physician offices that might not have the freezers needed for the other vaccines, public health officials say.
But the Johnson & Johnson shot also has a lower efficacy rate, leading some public health experts and government officials to worry that it will be viewed as substandard comparedwith the other vaccines. The Johnson & Johnson efficacy rate is 66% overall and 72% in the United States in preventing moderate to severe cases of covid-19, the disease caused by the coronavirus.
The vaccines by U.S. pharmaceutical giant Pfizer and its German partner BioNTech and by the biotech company Moderna are about 95% effective following their two-shot regimens.
Nirav Shah, director of the Maine Center for Disease Control and Prevention, said he is already getting tweets and emails from people expressing reservations. “The gentle ones say, ‘Is it okay if I get J & J, or should I wait for Pfizer?’ ” he said. “The strong ones say, ‘I don’t want J & J. I want Pfizer.’ “
Shah said he responds by saying all three vaccines have been shown to be fully effective in protecting against what people fear most – hospitalizations and death. And he notes that the two earlier vaccines were tested months before the emergence of “variants of concern,” including one first detected in South Africa that appears to affect the efficacy of the vaccines, so the results are not an “apples to apples” comparison. He urges people to get whatever vaccine they can.
Shah said he is planning to equip public health nurses and other vaccinators with the Johnson & Johnson vaccine and send them to far-flung corners of his state. “J & J will open up a new wing in our vaccination efforts – not just more people, but harder-to-reach people,” he said.
Jeanne Marrazzo, an infectious-disease doctor at the University of Alabama at Birmingham, placed the newest coronavirus vaccine in the context of vaccines used to thwart other infectious diseases.
“In a normal world, people would be jumping up and down for a vaccine that is more than 70 percent effective,” she said, noting that the FDA’s efficacy requirement is 50%. Instead, she said, “Some people are saying, ‘I am going to wait until I get the good vaccine.’ “
She doesn’t want the residents of Alabama’s rural areas – which tend to be less affluent and have a significant percentage of African Americans – to feel they are getting shortchanged if Johnson & Johnson’s product is deployed there.
“It’s something you have to think about as you make vaccines available because people are making comparisons,” Marrazzo said.
Paul Goepfert, director of the Alabama Vaccine Research Clinic and one of the scientific leaders of the Johnson & Johnson trial, said emerging evidence in the United Kingdom shows that the protection provided by the vaccine is similar to that from a single dose of Pfizer.
“Dose for dose, this vaccine is as good as any of the other ones,” he said. “I think the messaging needs to be this vaccine is comparable to the other two vaccines, and as soon as you have the availability [to take any vaccine], you should take it.”
But some experts say it is important for people to understand there might be differences between vaccines in preventing moderate cases of covid-19, because even those infections could have long-term consequences. At the same time, some doctors say they are encountering people saying they prefer the Johnson & Johnson vaccine because they don’t want to have to get a second shot.
For now, consumers are unlikely to have a choice of vaccines because there simply isn’t enough supply. That is poised to change in coming months. Pfizer-BioNTech and Moderna have committed to delivering a total of 220 million doses by the end of March. They say they have solved manufacturing challenges and are in a position to overcome scarcity that has hampered the nation’s fight against the coronavirus.
Some experts expect the United States will reach an inflection point by late spring, with more shots available than people who want to get them. A vaccine developed jointly by the University of Oxford and AstraZeneca and another from Maryland biotechnology company Novavax are also in the late stages of testing, and the United States has contracts for 400 million doses, if the vaccines are successful.
The addition of the Johnson & Johnson shot will diversify the nation’s portfolio of vaccines, adding one that works through a different scientific technology.
The Pfizer-BioNTech and Moderna vaccines employ an approach that had never been used in people outside of clinical trials. They deliver a strip of genetic material called messenger RNA carrying the instructions to build the spiky protein found on the outside of the virus.
In contrast, the Johnson & Johnson vaccine uses a harmless cold virus to deliver a gene encoding the spike protein to cells. The approach is more established. In both cases, cells follow genetic instructions to construct the spike, and the immune system learns to recognize the real thing from these replicas – and to respond.
The latest vaccine will also add a new supply stream to help alleviate shortages or manufacturing delays. A different process and supply chain are used, which could help bolster confidence that if any of the vaccines runs into production difficulties, there will still be supply.
“It’s always better to have that – if one vaccine gets in trouble for some reason or isn’t being produced at a high enough rate. That’s the most common problem we see when a new vaccine is produced: shortages,” said Nancy Bennett, professor of medicine and public health sciences at the University of Rochester School of Medicine and Dentistry. “The more the merrier.”
The advantages of each vaccine against the pathogen are still being untangled. Although a single shot of the Johnson & Johnson vaccine didn’t trigger antibody levels to soar sky high, it offered good protection against variants. Scientists think that could be because the vaccine robustly triggered another arm of the immune system, T cells, that may provide a different layer of protection.
Johnson & Johnson’s Janssen Pharmaceuticals unit applied to the FDA for emergency use authorization for the vaccine Feb. 4, submitting clinical trial data involving 44,000 participants in eight countries. On Wednesday, the agency released its analysis that the vaccine was safe and effective. On Friday, the agency’s outside vaccine advisers voted unanimously to recommend authorization.
The Centers for Disease Control and Prevention is scheduled to have an emergency meeting Sunday to review the safety and efficacy data and to recommend who should get the vaccine.
Meanwhile, vaccine makers in recent days announced progress on work designed to counter viral variants.
Moderna said it has made a new version of its vaccine targeting the variant first identified in South Africa. A small amount of vaccine has been sent to the National Institutes of Health for a trial to determine whether boosting humans with the modified vaccine will stimulate a strong immune response, the company said.
Pfizer and its partner BioNTech said they have started testing a third dose of their original coronavirus vaccine to see how well it protects against variants. They are also doing work aimed at variants of concern.
For scientists who have long worked on vaccines, the scale and velocity of the coronavirus research has been stunning. Goepfert, an HIV researcher who worked on the Johnson & Johnson trials, said the HIV vaccine trials he has worked on might have had as many as 5,000 participants, but the Johnson & Johnson study recruited 44,000 people in about 2½ months.
“What’s fascinating about covid vaccine studies is at first we were worried about enrolling the right kind of people at risk. But everybody’s at risk. You just needed to enroll people,” Goepfert said. “I think that’s sadly what helped us get these vaccine end points.”
The Johnson & Johnson study also might help elucidate some questions that are beginning to arise from real-world use of the vaccines. Goepfert said there were health-care workers in the trial who received the Johnson & Johnson vaccine but then became eligible for an authorized vaccine midway through and received one of the messenger RNA vaccines. Scientists have continued to collect safety data on those people, which should help show whether there are obvious risks from the mixing and matching that may begin to occur in the future, particularly as companies begin testing additional booster doses as a way to protect against variants.
For Helen Boucher, an infectious-disease doctor at Tufts Medical Center in Boston, the events of the past several weeks have been both devastating and exhilarating.
“We have hit this unfathomable number of people who have died and just thinking about it is overwhelming,” she said. At the same, she noted, hospitalizations and deaths are declining and vaccinations are increasing.
“I feel like there is light ahead,” she said. “I think the data supports it.”
Dermatology experts at the Department of Medical Services said on Wednesday that cats may transmit fungal disease to humans.
Dr Somsak Akksilp, the department’s director-general, said fungal disease usually causes a red rash that may leave black marks on the skin, which takes a long time to fade.
“Other furry animals like dogs and hamsters may also transmit fungal disease,” he said.
Dr Mingkwan Wichaidit, director of the Institute of Dermatology, said the fungus commonly found in cats is Microsporum canis, which can give humans an itchy rash.
“The most vulnerable to fungal disease are children, the elderly and those with low immunity,” she said, adding that people with fungal disease should see the doctor immediately.
“To prevent transmission, people should wash their hands after touching their pets, have them vaccinated and take good care of their pet’s fur,” she said. “Pets should also immediately be taken to the veterinarian if they develop a rash or start losing fur.”

 เมนูซื้อง่ายขายคล่อง “น้ำเต้าหู้” กินในปริมาณเท่าไหร่จึงส่งผลดีต่อสุขภาพ และเครื่องดื่มนี้จะช่วยลดความอ้วน ลดไขมัน ดีต่อระดับน้ำตาลในเลือด ระดับอินซูลินในเลือด และการย่อยอาหาร จริงหรือ!!
เมนูซื้อง่ายขายคล่อง “น้ำเต้าหู้” กินในปริมาณเท่าไหร่จึงส่งผลดีต่อสุขภาพ และเครื่องดื่มนี้จะช่วยลดความอ้วน ลดไขมัน ดีต่อระดับน้ำตาลในเลือด ระดับอินซูลินในเลือด และการย่อยอาหาร จริงหรือ!!