Months into the pandemic, still no easy answers on coronavirus testing
Health & BeautyAug 30. 2020Technicians process coronavirus saliva tests at the Waksman Institute of Microbiology in Piscataway, N.J. CREDIT: photo for The Washington Post by Bryan Anselm.
By The Washington Post · Rachel Weiner, Steven Mufson, Laurie McGinley · NATIONAL, HEALTH, HEALTH-NEWS As a new school year dawns, the demand for cheaper, faster and more accessible coronavirus testing is growing. But slow and sometimes erroneous test results and confusion over when and how to get tested continue to plague Americans as they wrestle with decisions about resuming their lives.
An abrupt government recommendation this week that fewer people get tested – while at the same time the Trump administration moved to purchase 150 million rapid tests – has made a disorganized testing regime even murkier.
Saliva tests are prepared for processing at the Waksman Institute in Piscataway., N.J. CREDIT: photo for The Washington Post by Bryan Anselm.
The controversy sparked by the revised standards and, separately, the fraught decisions about testing that confront local school officials and university administrators open a window onto the persistent problems dogging testing in the United States.
“I started to talk to colleagues nationally, and I was taken aback that most [public school] districts and most charter networks really had thrown in the towel quickly and said testing was too expensive and too complicated,” said Laura Clancy, chief talent officer for a nonprofit charter school network in Philadelphia and Camden, N.J., that plans to open its 24 schools on a limited basis by Oct. 1 pending community transmission rates and local guidance.
Some universities are already closing their campuses because they can’t keep up with outbreaks. A growing chorus of scientists say occasional screening, or surveillance, is not enough; they say students and others need be able to screen themselves at least twice a week.
While President Donald Trump has declared that we have enough or even too much testing, Democratic presidential nominee Joe Biden promised in his convention speech that “if I’m president . . . we’ll develop and deploy rapid tests with results available immediately.”
Political rhetoric aside, testing companies and policy advocates face regulatory, scientific, logistical and ethical hurdles more than half a year after the virus appeared in the United States.
Turnaround times for most tests have improved in recent weeks, in part because of a substantial drop in the number of tests administered. Still, the Trump administration estimates that over the past month, 1 in 5 tests took more than three days to come back – rendering results largely useless. The equipment needed at the nation’s biggest private lab companies is expensive and on back order.
Many companies have developed faster, cheaper tests, but there is a trade-off: Such tests are not nearly as sensitive as the standard coronavirus tests that can take days or weeks to process. The Food and Drug Administration is opposed to letting people take these tests at home unless they meet higher senstivity standards, fearing they would create a false sense of security. And public health experts remain deeply divided.
Testing serves two purposes. One is diagnostic, in which it is used to confirm the presence of the virus in people who have symptoms or a known exposure to someone who is already sick. The other is to detect people who are infected but don’t know it. That second purpose is especially important for screening asymptomatic people out of large groups, at schools and elsewhere.
Two kinds of tests exist to look for active infections. Molecular tests search for the virus’s genetic material. Antigen tests look for spiky proteins on the surface of the virus.
The gold-standard test is molecular – a polymerase chain reaction (PCR) test performed with a long nasal swab, known to be highly sensitive because of an expensive and time-consuming amplification process that finds even a small bit of infectious material.
Antigen tests are simpler and cheaper but less sensitive; they need more virus in the body to generate a positive result.
The White House just announced a deal to produce 150 million new rapid tests that yield results in 15 minutes, without added equipment. But these tests still must be analyzed by a medical professional. Technically they are approved for use only on people with symptoms, although the White House is touting them as a potential solution for schools and businesses.
That announcement came days after the introduction of new guidance on testing from the administration. It replaces advice that everyone who has been in close contact with an infected person should get tested to find out whether they had contracted the virus. Instead, the updated guidance says those without symptoms “do not necessarily need a test.”
Some experts argue the only way out of our current morass is testing that is even cheaper and simpler, performed entirely at home – even if it is not as sensitive.
“This can work better than a vaccine if it could just be produced at scale,” said Michael Mina, a Harvard University epidemiologist who has become a vocal advocate for rapid at-home testing. The tests “are not going to tell you if you definitely do or do not have any virus in you. And that’s not their role. They’re going to tell you if on a given day when you wake up and use this test inside of your house, you are at risk of transmitting the virus to other people.”
– – –
The novel coronavirus is particularly difficult to contain because it has a long incubation period and often leaves no symptoms behind. A test could be taken too early to catch the virus, or the results could come too late, when a person is already infecting others.
That’s why some public health experts argue in favor of rapid tests: If they’re cheap and convenient enough, they could be taken repeatedly by the same person, something unlikely to happen with more expensive PCR testing.
While the rapid tests might not catch every infection, experts say they should detect the most contagious cases.
“The notion of what a ‘junk test’ is has to be adapted for the role it’s playing,” said Carl Bergstrom, a biologist at the University of Washington and another proponent of rapid at-home testing. “It’s a substantial shift in what you’re looking for.”
Bergstrom suggests the FDA develop a separate track for approving such tests, with lower standards and appropriate warnings. People who are sick and need the right treatment, or who know they were exposed to the coronavirus, could get highly accurate PCR tests. Everyone else would proactively take rapid tests, using them as a potential indicator of infection.
An FDA official speaking on the condition of anonymity to explain the administration’s thinking said the agency is willing to approve less-sensitive rapid tests that are performed at point-of-care sites, such as a clinic or pharmacy, where a medical professional can offer advice on how to interpret the results. But the agency is loath to open the floodgates to rapid tests performed completely at home.
“Random testing of healthy people just all over the country is not what we’re advocating,” Adm. Brett Giroir, who leads the White House testing efforts, told reporters recently.
Some critics view even the few antigen tests that have met the FDA’s standards as suspect.
“It is better to not test at all and practice social distancing than to deliver a high number of false-negative results, since negative results often lead individuals to engage in risky behaviors that could increase virus spread,” said Bob Terbrueggen, president of a Los Angeles genomics company called DxTerity.
Public health experts express concerns that tests taken at home will go unreported, undermining efforts to measure the scope of the pandemic. Already, some states don’t report positive antigen test results, resulting in an incomplete portrait of the disease’s spread.
With no clear standards, average Americans may be on their own in understanding how best to use these tests.
“You’re potentially making consequential decisions, on the individual level, based on test results that are going to be harder to interpret,” Jennifer Nuzzo, an epidemiologist at the Johns Hopkins Center for Health Security, told reporters recently.
– – –
There are already more than 150 coronavirus tests approved for use by the FDA, with little explanation for consumers about what differentiates them.
One school district in Florida’s Lake County, for example, decided to screen all teachers and students before the school year began, partnering with a clinic that ended up choosing a rapid antibody test because other options were unreliable or not feasible.
“If you were to see my office . . . there’s boxes of rapid tests that we chose not to use,” said Matt Cady, practice administrator at Adult Medicine of Lake County. Some antibody tests were recalled by the FDA before they even arrived, while other options gave negative results in people known to be infected.
To cut down on lab time and boost capacity at the nation’s big labs, the FDA has approved efforts to pool samples and test groups of them at once, something the administration says at least half of states are doing. But pooling samples works only if most samples test as negative; a positive result means the whole batch needs to be tested again.
Peter Iwen, director of the Nebraska Public Health Laboratory, was one of the first scientists in the country to start pooling samples. Now, he says it’s pointless in his state: “The positivity rate in Nebraska is much too high,” he said.
The laboratory testing world is dominated by big companies – including Abbott Laboratories, Quest Diagnostics and Laboratory Corp. of America – that carry out about half of U.S. testing. Each machine is costly and processes as many as 2,000 tests a day. The American Clinical Laboratory Association, a trade group, says its members need Congress to establish a federal fund to pay for machines and tests not covered by insurance.
The rest of the testing world is full of small companies.
One called E25Bio in Cambridge, Mass., while still hoping to see its cheap at-home test hit the market, is now aiming for approval with a more sensitive version that requires a lab step.
“These type of antigen tests, while they will never be as accurate and sensitive as PCR, what they are very good at is detecting high viral loads early in infection,” E25Bio spokesman Carlos Henri-Ferré said. “What we’re talking about is a contagion tracker, a contagion stopper.”
Other companies are trying to bypass the debate with affordable, at-home saliva tests that can meet the FDA’s standards.
One is an antigen test being developed by a company in Hawaii named Oceanit, currently in clinical trials at The Queen’s Medical Center in Honolulu. Oceanit chief executive Patrick Sullivan said that by designing a molecule specifically for the coronavirus antigens, the test achieves greater sensitivity. The current model costs $20, but broader manufacturing could bring it down to $4 or $5, he said.
The company designed the test to be simple enough for 8-year-olds to take before school, but the first clients would be a different unruly bunch: mainland tourists.
“The restaurants, the hotels, the airlines – everybody wants a tool like this,” Sullivan said.
The FDA this month granted emergency use authorization for two saliva-based tests that don’t require swabs or the chemical testing agents that have been in short supply. The administration is encouraging schools to look into using both. While saliva tests are less common, researchers have found they can be as sensitive as nasal swabs.
SalivaDirect, developed at the Yale School of Public Health with funding from the National Basketball Association, cuts costs down to the level of a cup of coffee – $1 to $4 a test in part by avoiding costly preservatives and using a cheap container. The school is making its test available to any company or laboratory interested in using it.
“Its novelty is its simplicity,” said Anne Wyllie, a Yale epidemiologist. “We saw the need for cheap testing because it needs to be accessible around the country. And colleges and schools need frequent testing.”
But materials are not the only reason coronavirus tests are hard to come by. Andrew Brooks, a geneticist who runs a Rutgers University lab that in April got the first FDA emergency clearance for a saliva test, said even cheap and fast tests involve staffing and packaging costs. Tests need to be logged, billed and reported to public health authorities.
“What people don’t understand is there are other operational issues that impact the ability for the lab to do this, not just reagents,” said Brooks, whose lab has analyzed some Major League Baseball tests. “We can’t hire people fast enough.”
Back in Cambridge, not far from E25, a company called Sherlock Biosciences is developing a paper strip test that offers “lab quality molecular diagnostics in the palm of your hand,” in the words of chief executive Rahul Dhanda. Rather than searching for a protein, the test uses the virus itself to create a signal detectable without amplification or special instruments. By next year, Dhanda said, the company could produce a test with “as good or better sensitivity than exists with PCR today.”
But he said Sherlock Biosciences was wrestling with the value of holding out for perfection in the middle of a crisis. At the same time, he worries that sacrificing accuracy, even if allowed by the FDA, would make the test harder for people to use, understand and trust.
“We wonder whether we should be making some trade-offs on performance to get the products out faster,” he said. “We’re torn as to what the right answer is. And I think we’re all collectively as a sort of society trying to get to that.”
Amazon’s creepy new health wearable analyzes your voice and body
Health & BeautyAug 28. 2020The Halo app uses photos you take of your body in minimal, tight clothing to estimate your body fat composition. CREDIT: Amazon
By The Washington Post · Geoffrey A. Fowler · NATIONAL, BUSINESS, TECHNOLOGY, FEATURES, HEALTH, HEALTH-FEATURES
I couldn’t pick just one crazy thing to say about the Halo, Amazon’s new wearable health gadget. So here are three:
1. Mirror, mirror on the wall, Amazon thinks you’re fat.
2. The artificial intelligence would like you to stop sounding overwhelmed now.
3. That nagging voice inside your head is now on your wrist.
Amazon’s Halo Band and app track the wearer’s fitness, health and even emotional state. MUST CREDIT: Amazon
The Halo is a $100 wrist-worn device that, among other functions, listens to your conversations so you can understand how you sound to others. And it comes with a companion app that 3D-scans your body to track your progress at gaining your quarantine-15.
Amazon is upfront about these invasive functions, which users of the Halo have to opt into using. What’s revealing is that one of tech’s biggest companies thinks consumers in 2020 might want them.
The Halo uses microphones on its band to listen to snippets of conversation and analyze how it thinks you come across to others. CREDIT: Amazon
Amazon CEO Jeff Bezos owns The Washington Post, but I review all tech with the same critical eye. Amazon declined to let me speak with an executive about the product, nor did it offer me the chance to get my hands on one for first impressions. (Anyone can sign up for the product’s waiting list, and I did. Hope they pick me!)
It makes sense that Amazon wants to push into health. This year in particular, tech companies are trying to transition their body-worn devices from fitness trackers into health and wellness assistants. Earlier this week, Fitbit launched a new $330 smartwatch called the Sense that includes a temperature sensor, an electrocardiogram app and an electrodermal activity sensor to detect the body’s response to stress. In September, Apple is expected to unveil a new version of its Watch with more health bells and whistles.
The makers of Fitbits, Oura rings and other wearables have also been participating in clinical studies to see if the data they gather can be used to predict the onset of covid-19 symptoms before patients even realize they’re sick.
In some ways, Amazon’s Halo is a me-too health tracker. There’s no screen, but like Fitbits it has sensors that collect data about your activity, sleep, temperature and heart activity. Covered in fabric or silicone, the water-resistant Halo Band looks like a style of bracelet that might have been popular in high school in the 1980s. Its accompanying app and paid service nudge you to healthier habits with content from companies including Headspace and Orangetheory Fitness.
Unlike the Apple Watch and other devices, Amazon’s Halo hasn’t received Food and Drug Administration clearance for any of its functions. It doesn’t count as a medical device.
But the Halo and Amazon’s $4-per month service attempt to use AI to be a more “comprehensive” wellness guide – and that’s where things get weird. The Halo can’t track your weight on its own, but it asks you to take photos of your body (wearing minimal, tight clothing) with its app so it can estimate your body fat percentage. A motivational slider in the app shows you what you would look like if you lost weight.
And then there’s the tone-monitoring. Amazon says understanding emotion is key to overall health, so it uses AI to analyze “energy and positivity” in a customer’s voice recorded from microphones on the band. (It knows your voice, as opposed to those around you, by making a profile of you speaking.) Amazon says tone results may, for example, “reveal that a difficult work call leads to less positivity in communication with a customer’s family, an indication of the impact of stress on emotional well-being.”
Say what? Why would you want to know what an AI thinks about your tone? Are you supposed to make behavior changes – or seek counseling? Amazon says you could use it for feedback on public speaking, or to understand how sleep impacts your tone.
Amazon spokeswoman Molly Wade said its tech does not make “judgments” about tone, but determinations such as “friendly,” “hesitant,” and “overwhelmed” sure sound like judgments to me.
Also, why should we trust what AI has to say about this? The whole idea of “tone” is fraught with ideas about gender, ethnicity and class. Will it judge women more harshly than men? Amazon’s Wade says the company trained its system with data from “all demographic groups.”
Privacy is also clearly a stumbling block. Many owners of Amazon’s popular Echo speakers are, rightly, concerned the Alexa assistant is eavesdropping on their conversations. (Police are increasingly turning to those recordings for evidence.) Unlike Echo speakers, the Halo doesn’t send Amazon the words you say – instead, it listens on the band itself, where it runs an analysis of your tone and then deletes the files. (You can press a button on the band to deactivate its microphone.) Amazon says body scan images are sent to its cloud but are deleted from its computers after processing.
But using the Halo does mean Amazon is going to learn even more about you. Amazon says no one can view your health data without your explicit permission, and it won’t sell it. The giant retailer also says it won’t use the data gathered by the Halo to sell you things. But it has already announced a partnership with health insurance company John Hancock to share your data for savings.
Amazon has a long history of being the try-anything company in consumer tech. It doesn’t have its own smartphone on the market, so it has to think outside the box. Over the years, I’ve reviewed Amazon products including a closet camera that judges your fashion sense (the now defunct Echo Look), a TV streaming box you operate via voice (the FireTV Cube), and most recently glasses that let you have private conversations with Alexa everywhere you go (the Echo Frames).
Like many of those other Amazon product launches, you can’t just buy the Halo directly – at least not yet. Customers in the U.S. can sign up on Amazon’s website to request “early access” that includes the device and six months of service for an introductory price of $65.
Virus’s retreat in Brazilian Amazon upends notions of herd immunity
Health & BeautyAug 25. 2020Alessandra Said and her team take a 78-year-old covid-19 patient to an ambulance in the Coroado neighborhood of Manaus, Brazil, in May. CREDIT: photo for The Washington Post by Raphael Alves.
By The Washington Post · Terrence McCoy, Heloísa Traiano · WORLD, THE-AMERICAS The hospital system was coming apart. Coronavirus patients were being turned away. Basic necessities – beds, stretchers, oxygen – had run out. Ambulances had nowhere to take patients. People were dying at home. Gravediggers couldn’t keep up.
The human destruction in the Brazilian city of Manaus would be “catastrophic,” physician Geraldo Felipe Barbosa feared.
But then, unexpectedly, it started to let up – without the interventions seen elsewhere.
Photo by: The Washington Post — The Washington Post
Hospitalizations of coronavirus patients plummeted in the state from a peak of more than 1,300 in May to fewer than 300 in August. Excess deaths in Manaus fell from around 120 per day to practically zero. The city closed its field hospital.
In a country devastated by the novel coronavirus, where more than 3.2 million people have been infected and over 105,000 killed, the reversal has stunned front-line doctors. Manaus never imposed a lockdown or other strict containment measures employed successfully in Asia and Europe. And what policies did exist, many people ignored.
In the spring, the Amazonian city became a global symbol of the devastation the disease can wreak in the developing world. But now it has returned to near normalcy – far sooner than many expected – and scientists and public health officials are asking why. The question is part of a broader debate among scientists and public health officials over the mechanics of herd immunity and the level of transmission that must be crossed before the disease starts to recede.
European cities that were pummeled by the disease have begun to reopen without crippling second waves. In Guayaquil, the Ecuadoran metropolis where bodies were left on the streets, scientists have cautiously speculated that collective immunity has been reached. Some researchers are now suggesting the same about New York City.
The factors that are helping to keep the virus at bay in Manaus and other cities remain unclear. Changed behaviors and individual community characteristics surely play a role. Manaus is testing far more than it once did. But whatever the dynamic, scientists and health officials are starting to wonder whether early prognostications about herd immunity overshot the mark.
It was initially believed that between 60 and 70% of the population needed to develop antibodies to reach collective immunity. But Guayaquil never broke 33%. Manaus, the capital of Amazonas state, never got past 20.
“Manaus is an interesting case, indeed,” said Jarbas Barbosa da Silva, assistant director of the Pan American Health Organization. “The hypothesis – and this is just a hypothesis – is that the peak we had in Manaus was very strong, and there was such widespread community transmission that it may have produced some kind of collective immunity.”
Draconian restrictive measures reduce the disease sharply, Barbosa said. But in Manaus, the reduction has been gradual, with a steady progression of new cases still arriving every day. That curve suggests the disease followed a “natural dynamic,” Barbosa said.
Manaus, he said, “paid a very large price” to get there. During the spring, it suffered three times as many deaths as normal. In all, the city of 2 million along the Amazon River buried some 3,300 people more than usual.
“This was not a strategy,” Barbosa said. “It was a tragedy.”
– – –
The idea of herd immunity has long been used to justify and explain the purpose of mass vaccination campaigns. Scientists would plug the disease transmission rate – or how many people one sick person infects – into a calculation to determine the percentage of people who should be inoculated. For particularly infectious diseases, such as measles, that’s as high as 95%. For others, it’s lower.
But researchers say collective immunity works differently in a live outbreak. The disease doesn’t simply vanish when a magic number is crossed. Instead, as the pool of potential victims shrinks, transmission decelerates until it’s gone. Containment policies can lower transmission further. But regardless of whether they’re adopted, once the pool of potential victims reaches a critical mass, an explosive resurgence is unlikely. Too many people would have already contracted the disease.
“In Italy, it struck the Milan region very badly,” said Tom Britton, a mathematician at Stockholm University. “But not Rome very much. If I had to bet money that there was a second wave, I would bet all of my money on Rome, rather than Milan.”
Britton and other researchers have been studying what’s known as “heterogeneity in susceptibility.” Early herd immunity models – and vaccination campaigns – have operated from the assumption that everyone’s the same. But individuals vary: Some people are more socially active, others are more physically vulnerable. Heterogeneity, researchers say, reduces the percentage of infection at which herd immunity may be achieved. The people most likely to get the disease and pass it on – the most socially active, the most susceptible – catch it first. But once they’re out of the pool of potential victims, the risk is less for everyone else.
“The effect of their immunity will be bigger,” Britton said.
In a paper published in Science in June, he and other researchers estimated that population heterogeneity shaves the coronavirus herd immunity rate to 43%. Others say it might be lower.
Gabriela Gomes, a mathematician at the University of Strathclyde in Glasgow, has scrutinized European cities overwhelmed by the disease. In a paper she wrote with nine other researchers, which hasn’t yet been peer-reviewed, she arrived at a striking conclusion: Herd immunity could be lower than 20%.
“Without immunity, you would have expected the cases to start growing very soon after interventions were lifted,” she said. “That’s what we were saying at the time: ‘It’s premature to lift interventions. Cases will start going up.’ But they didn’t. And in most cases, they continued going down. It was quite unexpected.”
But with the stakes so high – more than 770,000 dead worldwide and so much about the virus still unknown – many researchers have been reluctant to say whether they believe the worst in some of the hardest-hit cities has already passed. No one knows how long immunity lasts. The virus could mutate.
“In Manaus, maybe we’re done with it, and that’s it,” said Jeffrey Shaman, an environmental health scientist at Columbia University. “I would love that as well. But the reality is that it’s wishful thinking. It’s confirmation bias. We can’t pick evidence we hope is true. We have to be very careful about this because it could blow up in your face very quickly.”
– – –
Pietro Pinheiro Alves, a physician in Manaus, knows how quickly that can happen. Despite its physical remoteness in the rainforest, Manaus is one of Brazil’s most international cities. Drawn by a free-trade zone, companies from all over the world have put down roots in the Amazon. As the coronavirus spread worldwide, strains from China, Europe and the United States were soon circulating, unseen.
It didn’t take long for the patient surge to overwhelm the hospital system.
“People are dying in their houses,” Pinheiro Alves wept into the phone in early May, when things were at their worst. “They can’t get any help in the hospitals.”
He felt hopeless. People were still crowding the streets. Officials weren’t willing to impose a lockdown. In impoverished Manaus, where many already live on the brink, the mayor said it would lead to social chaos and violence. So Pinheiro Alves spent his off hours trying to jury-rig ventilators.
Manaus Mayor Arthur Virgílio Neto said he “fought for social isolation.”
“The attempt failed,” he said. “There wasn’t real social isolation. People still went out, and it wasn’t understood why. In the most difficult hours, I’d go to the field hospital, get stuck in a traffic jam and think, ‘Why aren’t people home? What are they doing out?’ “
Physician Uildéia Galvão saw the result: Every day, there would be a line of ambulances outside her hospital in central Manaus, each holding a patient in need of a bed. Sometimes they sat for hours, waiting for someone to die and relinquish their bed.
At the height of the city’s outbreak, there would be three or four lined up. Then one day, it was two. Then one.
“It was the first sign that the number of emergency calls were dropping,” Galvão said.
Intensive care units started to clear. Emergency coronavirus calls slowed, dropping from 2,410 in April to fewer than 180 in July. The wail of ambulances quieted. Some scientists said victory was in sight.
“Why Manaus will be the first Brazilian city to defeat the Covid-19 pandemic,” wrote a group of researchers from the Federal University of Amazonas.
Street activity returned to pre-pandemic levels. People flocked to the river to swim and party. Appeals to wear masks: widely ignored. Private schools opened up. Then public. Cases continued to number in the hundreds every day, but far fewer were serious enough to warrant hospitalizations.
“There isn’t a concrete explanation,” said Henrique dos Santos Pereira, a scientist at the Federal University of Amazonas. Maybe there’s an unseen biological immunity in the population. Or the city’s relative youth staved off the worst.
“The problem is that we don’t know how many people are susceptible,” dos Santos Pereira said. “In the beginning, we were thinking it was everywhere, but it doesn’t seem like the whole world is susceptible. . . . It is causing us to reconsider the theory of herd immunity.”
Virgílio, the mayor, hopes the scientists are right. The medical system in Manaus has failed once. If a second wave does come, he has little doubt what would happen.

 สถาบันมะเร็งแห่งชาติ เผยมะเร็งลำไส้ใหญ่และไส้ตรง พบมากเป็นอันดับ 3 ในเพศชาย และอันดับ 4 ในเพศหญิง แต่ละปีจะมีผู้ป่วยรายใหม่ประมาณ 12,000 คน
สถาบันมะเร็งแห่งชาติ เผยมะเร็งลำไส้ใหญ่และไส้ตรง พบมากเป็นอันดับ 3 ในเพศชาย และอันดับ 4 ในเพศหญิง แต่ละปีจะมีผู้ป่วยรายใหม่ประมาณ 12,000 คน
 ใครว่า “ไส้เลื่อน” เป็นได้เฉพาะผู้ชาย แพทย์ชี้ชัดไส้เลื่อนเกิดขึ้นได้ทั้งผู้หญิงและผู้ชาย เตือนคนยกของหนัก ผ่าตัดหลังคลอด เคยผ่าตัด เป็นกลุ่มเสี่ยง
ใครว่า “ไส้เลื่อน” เป็นได้เฉพาะผู้ชาย แพทย์ชี้ชัดไส้เลื่อนเกิดขึ้นได้ทั้งผู้หญิงและผู้ชาย เตือนคนยกของหนัก ผ่าตัดหลังคลอด เคยผ่าตัด เป็นกลุ่มเสี่ยง



 รู้หรือไม่ 1 ใน 5 ปัญหาสุขภาพของผู้สูงอายุไทย คือโรคข้อเข่าเสื่อม ปวดข้อ-ปวดเข่าเรื้อรังไม่หายเสียที แพทย์ผู้เชี่ยวชาญกระดูกและข้อ ชวนเช็กลิตส์ตัวเองกันหน่อย…ปวดแบบไหนเสี่ยงเป็นโรคข้อเข่าเสื่อม!!
รู้หรือไม่ 1 ใน 5 ปัญหาสุขภาพของผู้สูงอายุไทย คือโรคข้อเข่าเสื่อม ปวดข้อ-ปวดเข่าเรื้อรังไม่หายเสียที แพทย์ผู้เชี่ยวชาญกระดูกและข้อ ชวนเช็กลิตส์ตัวเองกันหน่อย…ปวดแบบไหนเสี่ยงเป็นโรคข้อเข่าเสื่อม!!
 นักกายภาพบำบัด แชร์ 6 ท่าบริหารแก้อาการปวดคอ-บ่า-ไหล่ ไล่ออฟฟิศซินโดรม
นักกายภาพบำบัด แชร์ 6 ท่าบริหารแก้อาการปวดคอ-บ่า-ไหล่ ไล่ออฟฟิศซินโดรม






 กรมการแพทย์ ชี้สัญญาณเตือนมะเร็งปอด แนะประชาชนตรวจคัดกรอง หากพบระยะเริ่มต้นและรักษาตั้งแต่แรกๆ ช่วยลดความเสี่ยงและการเสียชีวิตลงได้
กรมการแพทย์ ชี้สัญญาณเตือนมะเร็งปอด แนะประชาชนตรวจคัดกรอง หากพบระยะเริ่มต้นและรักษาตั้งแต่แรกๆ ช่วยลดความเสี่ยงและการเสียชีวิตลงได้
 Technicians process coronavirus saliva tests at the Waksman Institute of Microbiology in Piscataway, N.J. CREDIT: photo for The Washington Post by Bryan Anselm.
Technicians process coronavirus saliva tests at the Waksman Institute of Microbiology in Piscataway, N.J. CREDIT: photo for The Washington Post by Bryan Anselm. 
 The Halo app uses photos you take of your body in minimal, tight clothing to estimate your body fat composition. CREDIT: Amazon
The Halo app uses photos you take of your body in minimal, tight clothing to estimate your body fat composition. CREDIT: Amazon 

 Alessandra Said and her team take a 78-year-old covid-19 patient to an ambulance in the Coroado neighborhood of Manaus, Brazil, in May. CREDIT: photo for The Washington Post by Raphael Alves.
Alessandra Said and her team take a 78-year-old covid-19 patient to an ambulance in the Coroado neighborhood of Manaus, Brazil, in May. CREDIT: photo for The Washington Post by Raphael Alves.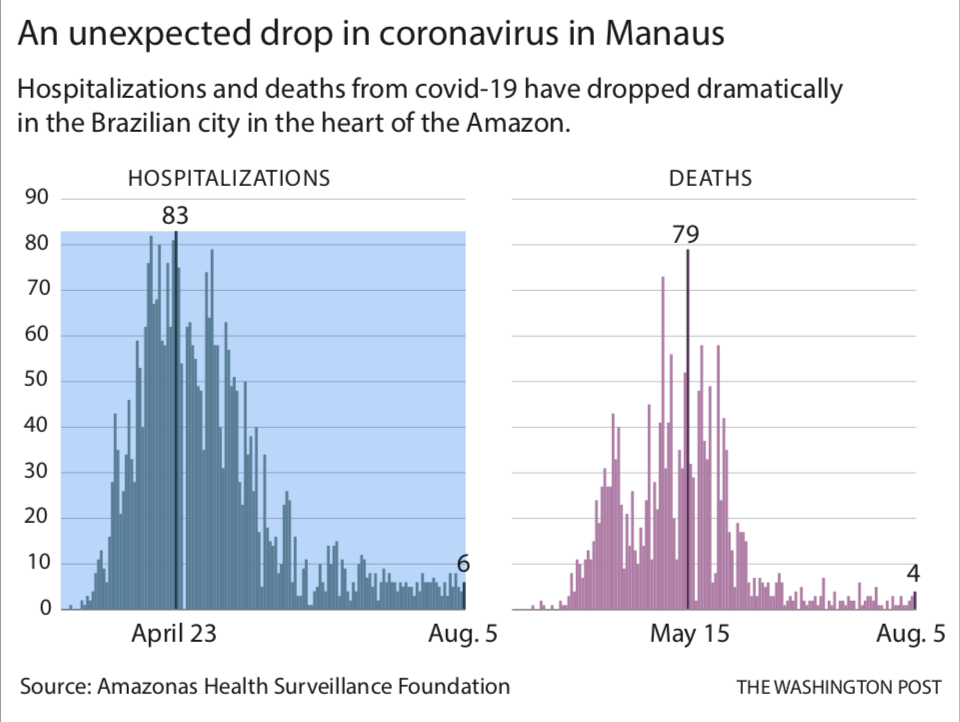
 ค้นหาสาเหตุของ “เหน็บชา” และอาการผิดปกติอื่นที่อาจมีร่วมด้วย พร้อมรู้วิธีป้องกันง่ายๆ จากการเลือกกินและการออกกำลังกายให้ถูกหลัก
ค้นหาสาเหตุของ “เหน็บชา” และอาการผิดปกติอื่นที่อาจมีร่วมด้วย พร้อมรู้วิธีป้องกันง่ายๆ จากการเลือกกินและการออกกำลังกายให้ถูกหลัก

 ว่าด้วยเรื่องของ “การนอน” หลับยาก หลับๆ ตื่นๆ หรือแค่เผลออดตาหลับ ขับตานอน ย้อนถามตัวเอง เพราะอะไร ทำไมถึงนอนไม่หลับ?
ว่าด้วยเรื่องของ “การนอน” หลับยาก หลับๆ ตื่นๆ หรือแค่เผลออดตาหลับ ขับตานอน ย้อนถามตัวเอง เพราะอะไร ทำไมถึงนอนไม่หลับ?

